This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. Is this acute STEMI? Is this an acute STEMI? -- Unlikely! The hypertension alone is the likely etiology of the pulmonary edema. He had no chest pain.
We discover that for STEMI/OMI vs subendocardial ischemia, we should look for STEMI(-)OMI, subacute OMI, and OMI in the presence of LBBB and RBBB, and consider the differential for diffuse ST depression with reciprocal ST elevation in aVR.
His vitals were within normal limits except some mild hypertension. Thus, this does NOT meet STEMI criteria (though, as of 2022, it is a formal "STEMI equivalent", assuming everyone agrees that this is de Winter morphology, for which there is currently no objective definition). He will be entered into the STEMI registry.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chest pain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
Written by Pendell Meyers, few edits by Smith A man in his 60s with history of stroke and hypertension but no known heart disease presented with chest pain that started on the morning of presentation at around 8am. So it is very unclear to me whether or not "posterior STEMI" is actually a recognized entity under our current guidelines.
Written by Pendell Meyers A man in his late 30s with history of hypertension, tobacco use, and obesity presented to the Emergency Department for acute chest pain which started approximately 3 hours prior to arrival, in the setting of a very stressful situation. Vitals were within normal limits except some hypertension. Which is true.
He had some cardiac risk factors including hypertension, on meds, but no previous coronary disease. He had an immediate ED ECG: There is artifact, but the findings appear to be largely gone now The diagnosis is acute MI, but not STEMI. His pain was intermittent and he was vague about when it was present and when it was resolved.
Written by Kaley El-Arab MD, edits by Pendell Meyers and Stephen Smith A 61-year-old male with hypertension and hyperlipidemia presented to the emergency department for chest tightness radiating to the back of his neck that has been intermittent for the past day or two. This ECG was read as “No STEMI” with no prior available for comparison.
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. See these posts: Chest Pain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab?
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
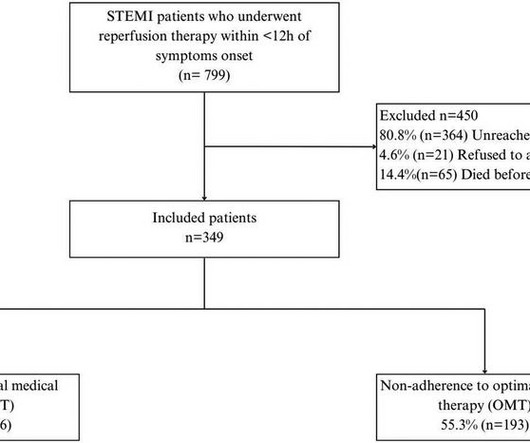
IntroductionIn developing countries, there is a notable scarcity of real-world data on adherence to optimal medical therapy (OMT) and its correlation with major cardiovascular adverse events (MACEs) after ST-elevation myocardial infarction (STEMI). Patients were followed up for 4.5 ResultsWe included 349 patients with a mean age of 58.08
Her vitals signs were remarkable for marked hypertension. would require the ST/S ratio to be 25% for diagnosis of STEMI in LVH. The physician was concerned about STEMI, but also worried that she was overreacting, with the potential that LVH was producing a "STEMI-mimic." The criteria of Armstrong et al. References 1.
He learned more about the patient: A 77 year old female with a past medical history of hypertension and hyperlipidemia presented to the ED at around 0520 after waking up at 0400 with 10/10 chest heaviness radiating to both arms. The patient had continued to have chest pain.
The Minneapolis Heart Institute Foundation (MHIF) is presenting leading research focused on trends in ST-elevation myocardial infarction (STEMI), the most severe form of a heart attack, at the American College of Cardiology’s Annual Scientific Session (ACC.24), 24), being held April 6-8 in Atltanta, GA.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Past medical history included diabetes and hypertension.
Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chest pain. This ECG is highly concerning for LAD occlusion despite it not showing a STEMI criteria.
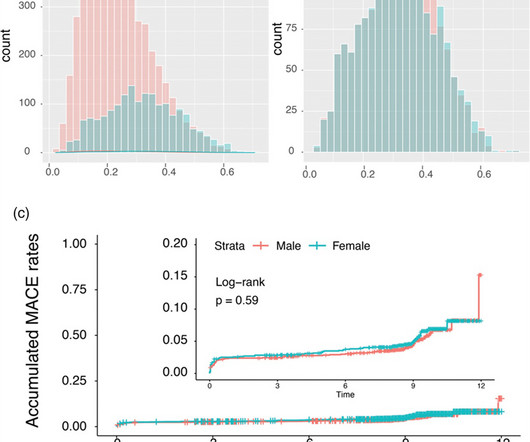
Purpose Construction of a prediction model to predict the risk of major adverse cardiovascular events (MACE) in the long term after percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardial infarction (STEMI).
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Immediate versus delayed invasive intervention for non-stemi patients. Is there anything else on the tracing to corroborate inferior OMI?
Written by Willy Frick with edits by Ken Grauer A woman in her 70s with a history of hypertension presented with acute onset shortness of breath. The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chest pain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. Patient still not having chest pain however this is more concerning for OMI/STEMI. Aspirin given. Am J Cardiol.
Sent by anonymous, edited by Pendell Meyers A man in his 50s with history only of hypertension presented with acute chest pain that started 45 minutes prior to presentation while doing yard work. Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI").
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chest pain and diaphoresis. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0.
The overall prevalence of arterial hypertension was 33.2%, hyperlipidemia, 26.9%, smoking, 17.8%, and diabetes, 3.9%. with ST elevated myocardial infarction (STEMI), 3.41% with unstable angina, 0.56% with stable angina, and 0.11% were diagnosed with various types of arrhythmias. Approximately 48.5%
It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI. A mong patients with STEMI, ventricular septal rupture is the most common and free wall rupture is the least common.
Written by Willy Frick A 67 year old man with a history of hypertension presented with three days of chest pain radiating to his back. The cardiologist agreed that the ECG was suggestive of STEMI, but the facility's cath lab was apparently not available and he therefore recommended emergent transfer to a cath capable facility.
After propensity-score-matching, primarily adjusting for age, hypertension and diabetes, our data revealed similar accumulated MACE in women and men (5.5% In the unmatched STEMI subgroup, all-cause mortality was significantly higher in females driven by older age (P < 0.001). vs. 3.9%; P = 0.020). vs. 5.2%; P = 0.749).
He stated that it is "an acute change from previous" in an elderly smoker with hypertension, syncope, and abdominal pain. However, there are morphologies of Takotsubo that cannot be distinguished from STEMI. Takotsubo This looks like and infero-posterior STEMI, but the QT is bizarrely long. Here are some examples: 1.
More past history: hypertension, tobacco use, coronary artery disease with two vessel PCI to the right coronary artery and circumflex artery several years prior. He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. Even the Queen can be wrong.
She is somewhat hypertensive, but her vital signs are otherwise normal. These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). While this may be change that is reciprocal to an Acute/Subacute Inferior STEMI, the problem is that LV aneurysm may also manifest with this reciprocal change. This case is tough.
The computer calls it a STEMI. Never chest pain but had to treat as hypertensive emergency. In fact, severe hypertension by itself can lead to greatly increased oxygen demand and type 2 acute MI, sometimes with ST Elevation. See this case of Type 2 STEMI due to severe hypertension. Here are more Type II STEMI.
This study investigates the relationship between baseline 5-HTP levels and the incidence of major adverse cardiovascular events (MACE) in patients who have experienced ST-elevation myocardial infarction (STEMI).Objective:Our Conclusion:Higher 5-HTP levels are independently associated with a reduced risk of MACE in patients after STEMI.
Will evolve into STEMI by prothrombotic trigger of lytic agent ECG will get normalised with clinical stability in some Nothing happens. Majority of Wellens end up as NSTEMI, statistics tells us about 20% of them can be STEMI in incognito mode demanding lysis or emergency PCI. ECG will remain same. How to manage Wellen syndrome?
A middle-aged woman with history of hypertension presented to another hospital approximately 2 hours after onset of chest pain and shortness of breath. This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." mm STE in V1 and 1.5-2.0
A middle-age woman with h/o hypertension was found down by her husband. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. With ventilations and epinephrine, she regained a pulse.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. I cannot be anything else.
This was sent to me by a French colleague, Olivier Peyronie "Yesterday we received a 62 yo man with diabetes, hypertension and smoker. Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." Time zero: What do you think?
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. BP was 110 and oxygen saturation was normal.
Steffen writes this case: "A few weeks ago I was able to recognize a STEMI because of what I had seen on your blog." "I He had no further risk factors for atherosclerosis besides hypertension. Steffen wrote: " I remembered the ECG from your blog titled: "STEMI Seen Best in PVC, Diagnosed by Medic, Ignored by Physician" from 2013.
The "criteria" for posterior STEMI are 0.5 Is it STEMI or NonSTEMI? The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis. The troponin I returned at 4.1 ng/mL (ULN = 0.030 ng/mL) , diagnostic of myocardial injury. mm STE in one lead.
A middle-aged woman with a history of hypertension presented with typical chest pain. Her BP was 160/80. Here was her presenting ECG, with chest pain: Inferior leads show hyperacute T-waves and reciprocal STD in aVL, with a reciprocally hyperacute T-wave in aVL. This is all but diagnostic of inferior OMI. There is also subtle STE in V1-V3.
Case An 82 year old man with a history of hypertension presented to the ED with chest pain at 1211. His EKG with worse pain now shows enough ST elevation to meet STEMI criteria. The EKG was read by the conventional computer algorithm as diagnostic of “ACUTE MI/STEMI”. There is pericardial tamponade.
A 50-something man with history only of alcohol abuse and hypertension (not on meds) presented with sudden left chest pain, sharp, radiating down left arm, cramping, that waxes and wanes but never goes completely away. Because we are hypnotized the STEMI paradigm. "If It was not a STEMI) 1. Symptoms were classic for MI 3.
I've previously discussed the interesting correlation of a qR pattern in lead V1 in patients with RVH — as strongly suggesting associated pulmonary hypertension ( See ECG Blog #234 and Blog #248 ). But limitation of this ST elevation to a single lead is not consistent with any distribution of a STEMI.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content