This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In tricuspid valve regurgitation, a complex condition that Cedars-Sinai experts regularly treat, the valve between two heart chambers on the right side doesn't open or close properly. Makkar explained the advances for patients with tricuspid valve disease in a conversationwith the Cedars-Sinai Newsroom. Image by Getty. Image by Getty.
The tricuspid valve (TV), historically deemed the ’forgotten valve’, is undergoing a renaissance as mounting evidence highlights its critical role in cardiovascular outcomes. Severe TR has been independently associated with increased mortality, regardless of left ventricular (LV) function or pulmonary pressures.
Tricuspid valve disease is an often underrecognized clinical problem that is associated with significant morbidity and mortality. Unfortunately, patients will often present late in their disease course with severe right-sided heart failure, pulmonaryhypertension, and life-limiting symptoms that have few durable treatment options.
BackgroundSevere tricuspid regurgitation (TR) causing cyanosis with patent foramen ovale (PFO) and right-to-left atrial shunting requires a precise diagnosis for optimal therapy. Tricuspid valve prolapse (TVP) can lead to TR and is sometimes overlooked, especially in complex cases with factors like pulmonaryhypertension (PH).
In Ebstein’s anomaly, there is downward or apical displacement of posterior and septal tricuspid leaflets. The anterior leaflet is not displaced, but is elongated to meet the other leaflets, so that when it closes, a loud sound, tricuspid sound, is produced, which is called as the sail sound.
Pulmonary arterial hypertension related to congenital heart disease as a paradigm of complexity Pulmonary arterial hypertension related to congenital heart disease (PAH-CHD) really represents a paradigm of complexity.
Pulmonary arterial hypertension (PAH) is characterized by increased pulmonary vascular resistance, imposing overload on the right ventricle (RV) and imbalance of redox state. PAH induction was implemented by a single dose of MCT (60 mg/kg i.p.). Treatment with SFN (2.5 mg/kg/day i.p.)
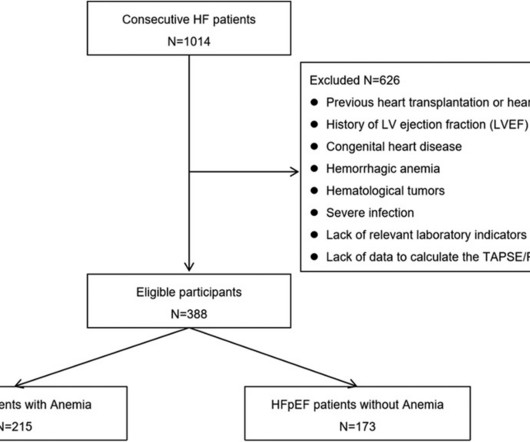
BackgroundPulmonary hypertension (PH) is highly prevalent in patients with heart failure with preserved ejection fraction (HFpEF), and it is a strong predictor of adverse outcomes. Both resting/stress TAPSE/PASP and TAS’/PASP were correlated with rest/exercise pulmonary capillary wedge pressure and mean pulmonary artery pressure.
Objective This study assessed the long-term effects of triple therapy with prostanoids on patients with pulmonary arterial hypertension associated with congenital heart disease (PAH-CHD), as there is limited information on the safety and efficacy of this treatment approach.
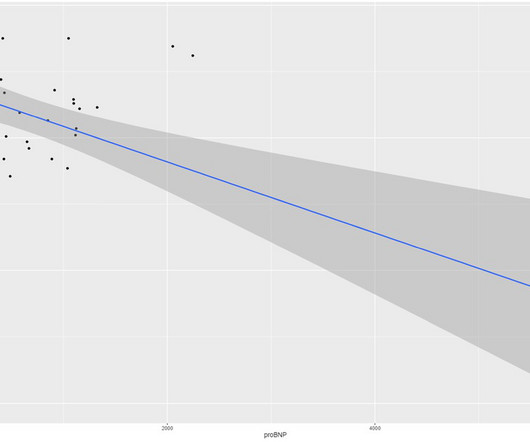
The level of hemoglobin (Hb) had a weak negative linear correlation with NT-pro-BNP (log-transform, r = 0.30, P < 0.0001) and a positively correlation with the tricuspid annular plane systolic excursion (TAPSE)/pulmonary arterial systolic pressure (PASP) ratio (r = 0.44, P < 0.0001).
Both atria develop from a combination of the primitive atrium, sinus venous, and pulmonary veins.It However, underlying lesions such as hypertension, mitral valve disease, COPD, ASD, and TR greatly influence the degree of atrial enlargement. But, we rarely dispute it , & ask which atrium dilates more in AF ? Let us see few factors.
(maybe not seen well on these echo-loops) The CW doppler at the tricuspid valve showed a maximum TR velocity of 2,55m/s with a TRP gradient of 26mmHg. large ASD, partial anomalous pulmonary venous return, significant tricuspid regurgitation, carcinoid valvular disease, etc,) 2) Conditions causing pressure overload of the RV. (E.g
Moreover, pulmonary artery pressures were ameliorated (estimated systolic pulmonary artery pressure: from 47.2±15.8 However, right heart dysfunction as well as the proportion of patients with severe tricuspid regurgitation remained unchanged. ±15.8 ±15.1 mm Hg, p value: 0.0079). to 84.7%) and 74.6% (95% CI 65.9%
Crochetage sign on ECG in ASD ECG in ASD with severe pulmonaryhypertension: Tall R’ in V1, ST depression in inferior leads and V2-V5, and T inversion in inferior leads and V1-V6 are seen. All these features together in a cyanotic congenital heart disease is characteristic of tricuspid atresia.
And that will be the approximate level of the tricuspid valve, the reference point for measuring right atrial pressure. In right atrial tracing, this occurs at the time of right ventricular contraction, with bulging upwards of the tricuspid valve. The Y descent is shallow in tricuspid stenosis, and absent in cardiac tamponade.
This suggests that there is pulmonaryhypertension and thus possibly RVH. Severe tricuspid regurgitation. --The The estimated pulmonary artery systolic pressure is 31 mmHg + RA pressure. That condition is tricuspid stenosis, which is rare. There is, however, a very peaked P wave in lead II (a "peaked P pulmonale").
Some of the other useful parameters are mitral E velocity deceleration time, changes in mitral inflow with Valsalva maneuver, mitral L velocity, isovolumic relaxation time, left atrial maximum volume index, pulmonary vein systolic/diastolic velocity ratio, color M-mode Vp and E/Vp ratio.
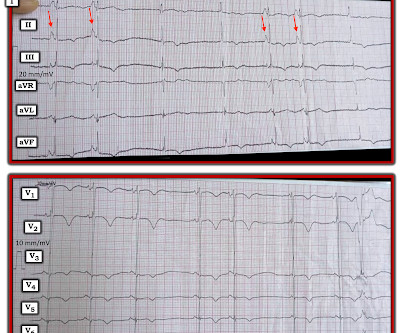
Perhaps the patient has pulmonaryhypertension and/or tricuspid regurgitation? RED arrows show what looks to be sinus P waves that are HUGE !!!! consistent with RAA (which is consistent with this patient’s underlying heart disease.
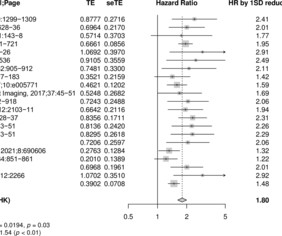
Background Right ventricular (RV) dysfunction is associated with adverse outcomes in patients with pulmonaryhypertension (PH). This systematic review and meta-analysis evaluated the prognostic value of RV free-wall longitudinal strain (RVfwLS), compared with other RV parameters in PH. HRs were standardised using the within-study SD.
BACKGROUND:Right ventricular-arterial coupling (RVAC) describes the relationship between right ventricular contractility and pulmonary vascular afterload. In a retrospective analysis, hybrid (echo and invasive) RVAC metrics included TAPSE/pulmonary vascular resistance (PVRi) and RVFW-LS/PVRi.
Edwards EVOQUE Tricuspid Valve Replacement System (Approved: 02/01/2024) This system provides a novel approach to tricuspid valve replacement, potentially benefiting patients with tricuspid regurgitation without open-heart surgery. March 2024 FDA Approvals: A Milestone Month for Cardiorenal metabolic Health 1.
Institutional Coronary Artery Bypass Case Volumes and Outcomes European Journal of Heart Failure October 2023 Makoto Mori 1 Robotic Mitral Valve Repair for Degenerative Mitral Regurgitation The Annals of Thoracic Surgery August 2023 Carlos Diaz-Castrillion 2 Volume-Failure to Rescue Relationship in Acute Type A Aortic Dissections: An Analysis of The (..)
Bernoulli equation (P=4V 2 ) gives the gradient of tricuspid regurgitation flow, which corresponds to the pressure difference between right ventricle and right atrium in systole. The early diastolic pulmonary regurgitation (PR) gradient (peak PR gradient) will give an estimate of mean pulmonary artery pressure.
Background Pulmonary endarterectomy (PEA) is the treatment of choice for chronic thromboembolic pulmonaryhypertension (CTEPH), while balloon pulmonary angioplasty (BPA) is an alternative for inoperable patients. The TAPSE/systolic pulmonary artery pressure ratio improved similarly in both groups.
In tricuspid valve regurgitation, a complex condition that Cedars-Sinai experts regularly treat, the valve between two heart chambers on the right side doesn't open or close properly. Makkar explained the advances for patients with tricuspid valve disease in a conversationwith the Cedars-Sinai Newsroom. Image by Getty. Image by Getty.
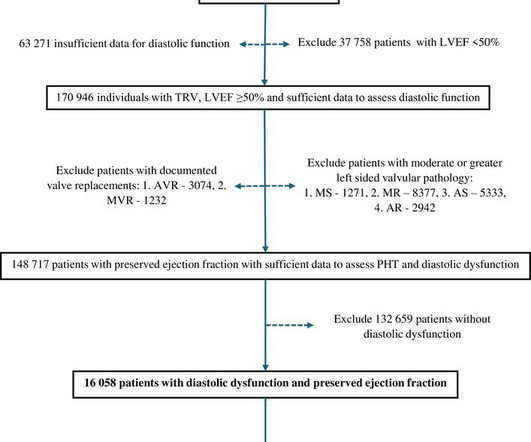
Aims Pulmonaryhypertension (PHT) appears to be very common in heart failure with preserved ejection fraction but details on its prevalence, severity and prognostic implications have not been well defined.
Background and objectives Left ventricular diastolic dysfunction (LVDD) is commonly associated with pulmonaryhypertension (PHT); however, the factors associated with the presence and severity of PHT in patients with LVDD have not been well characterised. Results Mean age was 73±12 years and 9216 (57.4%) were women.
Maximal tricuspid regurgitation velocity [2.9 m/s] and derived systolic pulmonary pressure [38 (29.544.5)mmHg] ConclusionChanges in cardiac function in the context of hypertensive pregnancy diseases can be observed with regard to various echocardiographic parameters. were found. mmHg] were borderline elevated.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content