This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
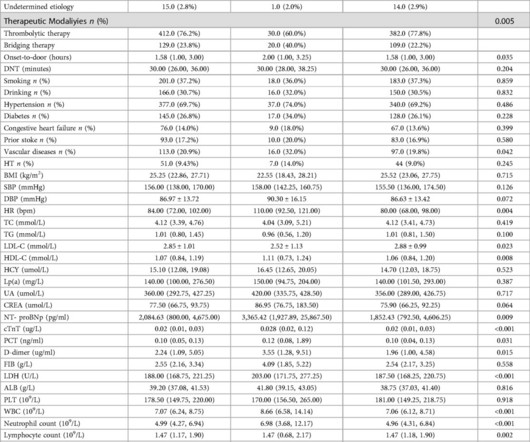
In-hospital mortality was defined as a Modified Rankin Scale (mRS) score of 6 point. Multifactorial logistic regression analyses using fully adjusted models, demonstrated that the SII is independently associated with the risk of in-hospital death. Notably, the combined model outperformed the SII alone (P<0.05).
Introduction:Emergency-department-based implementation strategies to increase thrombolysis are promising. We sought to quantify the number of hospitals with opportunities to increase thrombolysis under various tPA treatment thresholds.Methods:We used data from the 2018 State Inpatient Databases (SID) from 17 states.
SETRAC has demonstrated its efficacy in improving thrombolysis rates in patients with acute ischemic stroke. SETRAC stroke committee compiled and shared this data with the coordinators and hospital administrators on a quarterly basis. The rates of thrombolysis increased from 7.10% in 2014 to 11.8% in 2023 (p<0.001).
The SHINE trial , funded by the National Institutes of Health’s National Institute of Neurological Disorders and Stroke (grant U01 NS069498), was conducted at UVA Health and 69 other hospitals around the country. Of the 1,151 SHINE trial participants, 725, or 63%, underwent thrombolysis. Approximately 80% had type 2 diabetes.
We aimed to create a protocol that identifies thrombolysis candidates for patients presenting with isolated dizziness.Methods:A code stroke activation protocol was implemented by the Rhode Island Hospital Stroke Committee in 08/2021. hrs since LKW. From 01/2023-06/2024 there were 0 misses. in 2021, 37.5
Despite initiating thrombolysis for cerebral infarction and supportive treatments for heart failure, including VA-ECMO, the patient's condition continued to decline, evidenced by cardiogenic shock, heart failure, and progressive neurological deficits including coma and dilated non-reactive pupils.
Thrombolysis at the spoke hospital with the patient transferred to the hub for MT is a model known as drip-and-ship. Thrombolysis dwell time was defined as the timefrom administration of thrombolysis to repeat vascular imaging. The mean time from LKN to thrombolysis was 2.2 years (range, 25.1 range, 0 to 34).
Introduction:IV thrombolysis is a proven treatment for acute ischemic stroke (AIS), but it is still underutilized in real-world clinical practice. Trends in IV thrombolysis rate were respectively analyzed for all patients (cohort 1), patients who arrived at the hospital within 4.5
Introduction:Trials using advanced imaging have shown a benefit from intravenous thrombolysis in patients with wake-up stroke, but real-world data is limited. In this study, we compared discharge outcomes and hospital length of stay for patients with ischemic stroke selected for wake-up protocol with vs. without thrombolytic therapy.
Is primary PCI superior to thrombolysis in the first hour of STEMI ? The fact of the matter is, at best, pPCI fights for equipoise in the first hour, but thrombolysis is a clear winner in moral, scientifc & holistic perspective, as it can be administered very early, at a fraction of cost ,independent of expertise and infrastructure.
Objectives:To examine whether thrombolysis care metrics have improved in all races and ethnicities with the launch and advance of Target: Stroke (TS) national quality initiatives.Methods:This cohort study included patients presenting to Get With The Guidelines (GWTG)-Stroke participating hospitals within 4.5
Whether intravenous thrombolysis (IVT) is safe and effective for acute ischemic stroke (AIS) patients with CAA is largely unknown.Methods:This was an explorative analysis of a nationwide database of hospitalizations in the United States. 1.41], p=0.94) or in-hospital mortality (aOR 0.91 [95%CI 0.45-1.84], 4.16], p=0.001).
Introduction:The tenecteplase versus standard of care for minor ischemic stroke with proven occlusion (TEMPO-2) trial showed that patients presenting with minor deficits up to 12 h do not benefit from intravenous thrombolysis. h, if they were not eligible for standard-of-care thrombolysis. mg/kg) or non-thrombolytic standard of care.
Most respondents (88%) agreed there were barriers to acute stroke thrombolysis in the region. Among 51% of countries surveyed, no acute thrombolytic treatment was provided for acute stroke in the 2021 calendar year. Only 1 center treated >100 cases per year.
Background:Prior studies have shown that individuals who have an in-hospital stroke are less likely to receive thrombolysis. Few studies have investigated the trends of in-hospital strokes over time, and many large databases do not include in-hospital strokes. for in-hospital strokes and 13.4% in1993/94 (p=0.003).
Introduction:Current guidelines recommend 24-hours of high-intensity monitoring (HIM) for acute ischemic stroke patients post-intravenous thrombolysis (IVT) due to risk of bleeding complications including symptomatic intracranial hemorrhage (sICH). The median length of hospital stay for the HIM group was 49.8 hours [IQR: 43.8-83.3]
Stroke, Volume 56, Issue Suppl_1 , Page ATP20-ATP20, February 1, 2025. Patients with elevated traditional risk factors at admission may benefit more from thrombolytic therapy compared to those with high inflammatory response indicators.
Background:The benefits of endovascular thrombectomy (EVT) for posterior cerebral artery (PCA) occlusion remain controversial, but intravenous thrombolysis (IVT) has proven benefit across nearly all ischemic stroke types. to 2.87) with no difference in length of hospital stay (adjusted β 0.26, 95% -0.71
Findings from the highly-anticipated MOST (Multi-Arm Optimization of Stroke Thrombolysis) trial were presented on the first day of the American Stroke Association’s International Stroke Conference, ISC 2024, being held through Feb. 9 Phoenix, AZ. Adeoye, M.D.,
Introduction:Large vessel recanalization (LVR) is a well described phenomenon following intravenous thrombolysis (IVT). Stroke, Volume 56, Issue Suppl_1 , Page AWP3-AWP3, February 1, 2025. Clinical and radiographic information at the time of LVO diagnosis were collected.
Kulcsar, University Hospital Zurich milla1cf Mon, 02/26/2024 - 12:13 February 26, 2024 — Ischemic strokes are a major health burden. Contemporary treatments to remove the clot include intravenous thrombolysis or mechanical thrombectomy using a catheter. Image courtesy of P. Thurner und Z.
Background:Treatment options and outcomes in stroke also depends on pre-hospital delays. Compared to the patients who reached by non-EMS mode, patients who reached by EMS mode were more likely to receive intravenous thrombolysis (16% vs 44%,). Stroke, Volume 56, Issue Suppl_1 , Page AWMP53-AWMP53, February 1, 2025.
Background:Mechanical thrombectomy (MT) as treatment for acute ischemic stroke (AIS) has demonstrated superior functional outcomes compared to intravenous thrombolysis (IVT). Stroke, Volume 56, Issue Suppl_1 , Page ATP115-ATP115, February 1, 2025. Matched propensity scores were used to adjust for baseline differences across 36 factors.
Pre-hospital identification may increase and speed study enrollment.Methods:Midway through the Multi-Arm Optimization of Stroke Thrombolysis (MOST) trial, our mobile stroke unit research personnel monitored EMS radio for potential stroke patients en route to our study hospital. patients per month compared to 2.4
Introduction:In acute stroke patients who receive revascularization with endovascular thrombectomy (EVT) alone vs intravenous thrombolysis (IVT) followed by EVT, combination treatment has shown improved outcomes measured by the modified Rankin Scale (mRS). Stroke, Volume 56, Issue Suppl_1 , Page AWP256-AWP256, February 1, 2025.
Background:Patients with acute ischemic stroke harboring a large vessel occlusion (LVO) admitted to non endovascular-capable centers often require inter-hospital transfer for thrombectomy. Patients were included if they had evidence of an LVO at the referring hospital and had an NIHSS score documented before and immediately after transfer.
However, the true benefits are hidden in a timely early reperfusion, best done at out-of-hospital (or even in-hospital*) with the emergency crew’s assistance. In this context, we need a movement to revive the pre-hospitalthrombolysis. Efficiency of thrombolysis is highly reproducible.
Introduction:Telestroke has the potential to revolutionize acute stroke treatment by improving access to optimal stroke care, including time-sensitive care such as thrombolysis. presented 4 hours of last known well, no contraindications to thrombolysis). presented 4 hours of last known well, no contraindications to thrombolysis).
This review summarizes evidence from cardiology in this field and highlights the need of such measures to be incorporated in systems of care for stroke, and further information is needed to develop efficient systems of care at a regional and hospital level.
Blood was obtained on the MSU, in the hospital, and from healthy adult controls. Median initial NIHSS score was 6 (range 1-22; median hospital discharge NIHSS score was 1 (range 0-20). Twenty-three (88%) patients received IV thrombolysis and 7 (27%) had mechanical thrombectomy. Median lesion volume on MRI was 1.4
stroke center distribution is inconsistent across states, with around 77% of rural counties deemed "medical deserts" due to a lack of healthcare services.Methods:We conducted a comprehensive survey of hospitals in Oklahoma to assess accessibility to acute stroke therapies. In the U.S.,
Background:Every minute is crucial in treating acute ischemic stroke (AIS), as the effectiveness of intravenous thrombolysis and endovascular therapy is highly time-dependent. Stroke, Volume 56, Issue Suppl_1 , Page AWP70-AWP70, February 1, 2025.
Methods:Using the American Heart Association Get With The Guidelines-Stroke Registry from January 1, 2013 to December, 31 2021, we analyzed data on all ischemic stroke patients hospitalized and treated with IV-tPA. The primary outcome of interest was symptomatic intracranial hemorrhage (sICH) within 36 hours of tPA administration.
However, not all patients with strokes requiring intervention present to the hospital by ambulance, which would usually be the fastest means by which to reach a hospital. received thrombolysis and 53.6%
Subjects were divided into "intravenous thrombolysis group" and "non-intravenous thrombolysis group". Result:A total of 1971 patients (437 thrombolysis) were included. In the external validation set, the AUC-ROC values of "PAIST Scale" were 0.855 in the non-thrombolysis group and 0.778 in the thrombolysis group.
However, there is conflicting data in terms of intracranial hemorrhage risk.Objective: We are reporting the rate of symptomatic intracranial hemorrhage(sICH) in TNK and tPA treated stroke populations across two large hospital systems.MethodsDesign: Retrospective cohort observational study.
Background:Stroke patients with limited English proficiency (LEP) in the United States have limited stroke recovery and reduced post-stroke neurological care.Objective:Identify 90-day stroke outcomes using the modified Rankin Score (mRS) for patients discharged from Methodist Hospital with LEP. There were 55 identified as LEP.
Plan to follow‐up 2‐month post‐hospitalization for left ICA stenting.ConclusionWhile pre‐interventional IVT‐associated ICH in AIS with LVO are rare, few cases have been shown to have positive neurological outcomes [2,5,7]. Patient was discharged on Aspirin 81 mg daily to inpatient rehabilitation with NIHSS 21, mRS 4 (0 prestroke).
Secondary outcomes were in‐hospital mortality, intracerebral hemorrhage, and length of stay. P = 0.91), but there were longer lengths of hospital stay (adjusted β, 1.26; 95% CI, 0.78–1.74;P<0.001) P<0.001) and shorter hospital stay (adjusted β, −0.41; 95% CI, −0.63 P = 0.22).
We defined optimal destination according to the ASA algorithm, which recommends bypass for patients within 24 of last known well if large vessel occlusion suspected and bypass will not delay thrombolysis. Optimal hospital destinations were selected for 310/499 (62.1%) patients prior to the protocol and 86/117 (73.5%) after (p=0.021).
However, there is a paucity of population-based studies of the prevalence and effects of APLS diagnosis on patients hospitalized with IS. The primary outcomes were in-hospital death vs good outcome (discharge home/self care). We excluded individuals with ICD codes for other thrombophilia conditions (D6*). 0.78, p<0.001).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content