This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Then I always look to see if the initial deflection of the QRS has a lot of voltage change per change in time (seen in tachycardias that are initiated from above the ventricle because the propagate through fast conducting purkinje fiber. Tachycardia exaggerates ST Elevation in LBBB and Paced rhythm 5. Pacemaker mediated tachycardia!
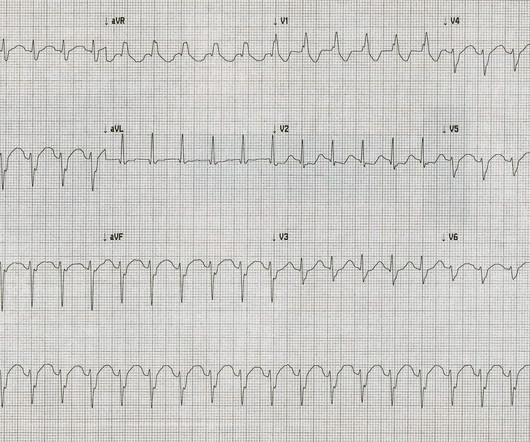
ECG#1 There is a regular tachycardia with a ventricular rate of about 180 bpm. Smith comment : When there is a regular wide complex tachycardia, first assess whether it is sinus or not. Put shortly is SVT with "Shark Fin STE" and not ventricular tachycardia. An ECG was recorded immediately and is shown below. Is there OMI?
male with pertinent past medical history including Atrial fibrillation, atrial flutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Description : Regular Wide Complex Tachycardia at a rate of about 160. SVT with aberrancy?
Of these, AA is one of the leading causes for hospital admissions in ACHD care. 1 Factors related to congenital heart disease, such as underlying anatomy, surgical repair technique and scars, can all be considered as AA substrates. Early diagnosis and ECG documentation is therefore essential for arrhythmia management.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
The ECGs show a wide complex, irregularly irregular tachycardia. This patient was admitted to the hospital and taken to the EP lab the following day. At that time, he presented via EMS and had received magnesium and lidocaine prehospital for concerns of ventricular tachycardia. 2 hrs later: Still sinus with subtler WPW.
The study provides real-world evidence that a wide range of patients can safely and effectively use the experimental drug, called etripamil, to treat recurrent paroxysmal supraventricular tachycardia (PSVT) episodes at home, potentially sparing them the need for repeated hospital trips for more invasive treatments.
The ECG in Figure-1 — was obtained from a middle-aged woman with positional tachycardia and diaphoresis with change of position from suprine to sitting. My THOUGHTS on the ECG in Figure-1: The rhythm is sinus tachycardia at ~105/minute ( ie, The R-R interval is regular — and just under 3 large boxes in duration ).
The 12-lead ECG and long lead II rhythm strip shown in Figure-1 — was obtained from a previously healthy, elderly woman who collapsed in the hospital parking lot. C ASE C onclusion : I lack detailed follow-up from today's case — other than knowing that the Atrial Tachycardia was controlled.
Alternatively, it could be posterior fascicular ventricular tachycardia. Either the PSVT was broken and restarted, or there is sinus tachycardia. Outcome: The etiology of the patient's sinus tachycardia was not discovered. He later returned to the hospital for recurrent bouts of idiopathic sinus tach.
Overall, patients' median length of hospital stay was 2 days (IQR, 22.5 There was no statistically significant difference between the two groups' median hospital stays [Group 1: 2 (IQR, 22.5) There was no statistically significant difference between the two groups' median hospital stays [Group 1: 2 (IQR, 22.5) Overall, 88.9%
The optimal timing for ventricular tachycardia (VT) ablation in reducing VT recurrence and improving patient survival is an important but unresolved topic.
For clarity in Figure-1 — I've reproduced today's ECG — obtained following successful resuscitation of out-of-hospital cardiac arrest. Confirmation of sinus tachycardia should be easy to verify when the heart rate slows a little bit ( as the patient's condition improves ) — allowing clearer definition between the T and P waves.
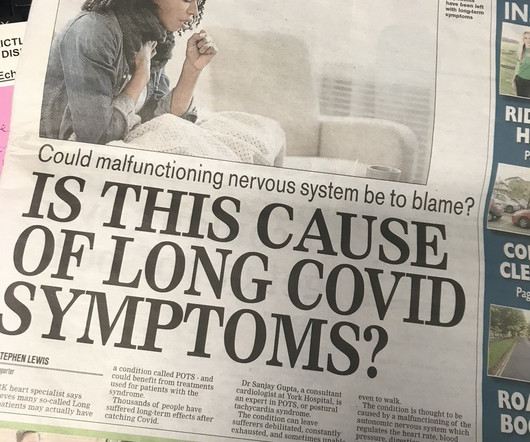
Dr Sanjay Gupta, a consultant cardiologist at York Hospital, is an expert in POTS, or postural tachycardia syndrome. The post York Hospital Consultant Could Have Treatment to Tackle Long Covid appeared first on Dr Sanjay Gupta Cardiologist. The symptoms can last for years, ruining patients’ lives. Read more here.
Recurrent symptomatic supraventricular tachycardia (SVT) can significantly affect patients’ quality of life and is a common cause of hospitalizations in the US. In light of its outstanding risk/benefit profile, catheter ablation (CA) is nowadays the recommended therapy for SVT and can be performed during hospitalization.
Catheter ablation for ventricular tachycardia (VT) has been shown to decrease the risk of VT recurrence and hospitalization. However, a critical gap exists in national-level data assessing its impact on hospital outcomes in patients with acute heart failure with reduced ejection fraction (HFrEF).
Wide-complex tachycardia: VT or aberrant, or "other?" A wide-complex tachycardia in an older patient must immediately suggest ventricular tachycardia. Sinus tachycardia with aberrancy was unlikely as the rate was consistently 150 bpm, without spontaneous variation. second ), in which the tachycardia is sustained.
A 50-year-old woman was referred to our hospital for catheter ablation of a regular narrow QRS tachycardia with a short RP interval. A narrow QRS tachycardia was reproducibly induced by programmed atrial extrastimuli with an AH interval jump. No retrograde dual atrioventricular (AV) nodal physiology was observed.
They had already cardioverted at 120 J, then 200 J, which resulted in the following: Ventricular Tachycardia They then cardioverted at 200 J which r esulted in the same narrow complex rhythm shown above, at 185 beats per minute. This would treat both SVT or sinus tachycardia. Henry Ford Hospital. Henry Ford Hospital.
Abstract Introduction Supraventricular tachycardia (SVT) is a common pediatric arrhythmia. Methods and Results This is a multicenter retrospective cohort study from three academic children's hospitals. Methods and Results This is a multicenter retrospective cohort study from three academic children's hospitals.
She had previously undergone three prior endocardial radiofrequency ablations for scar-related ventricular tachycardia (VT) with the most recent procedure at our center 4 months prior to the current hospital presentation.
A 15-year-old young male, presented to arrhythmia clinic with episodes of recurrent paroxysmal palpitations, lasting for several hours, requiring multiple admissions and DC cardioversion in the local hospital. What is the mechanism of the tachycardia? The 12 lead ECG (figure 1) and intracardiac recordings (figure 2) are shown below.
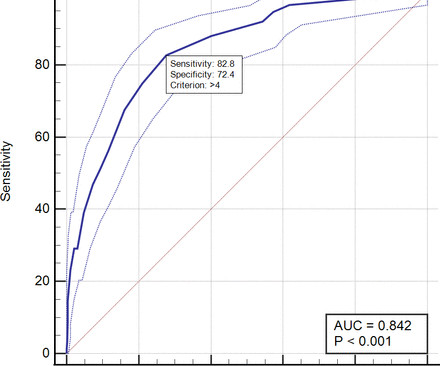
Background This study aims to develop PADjadjaran Mortality in Acute coronary syndrome (PADMA) Score to predict in-hospital mortality in acute coronary syndrome (ACS) patients based on clinical examination only. Conclusion PADMA Score is a simple scoring system to predict in-hospital mortality in ACS patients.
A few days into her hospital stay she developed chest discomfort and the following ECG was recorded. The ECG below was on file and was taken a few days earlier, on the day of admission to the hospital. The above ECGs show the initiation and continuation of a polymorphic ventricular tachycardia. What do you think?
She presented to an outside hospital after several days of malaise and feeling unwell. Sinus tachycardia has many potential causes. This is especially true for the elderly patient with sinus tachycardia. What is the cause of the sudden tachycardia? At the time of admission, her vital signs were normal.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Between 81-95% of life-threatening ventricular dysrhythmias and acute cardiac failure occur within 24-48 hours of hospitalization. Sinus Tachycardia ( common in any trauma patient. ).
Abstract Introduction Due to its unique features, pulsed field ablation (PFA) could potentially overcome some limitations of current radiofrequency (RF) ventricular tachycardia (VT) ablation. In case 1, during the in-hospital stay, ECG monitoring did not show VT recurrences.
The aim of this study was to describe incidental arrhythmias detected during screening for AF in the STAR‐FIB (Predicting SilenT AtRial FIBrillation in Patients at High Thrombembolic Risk) cohort study.Methods and ResultsIn the STAR‐FIB cohort study, we screened hospitalized patients for AF with 3 repeat 7‐day Holter ECGs.
Therefore, we sought to analyze the regional differences in the in-hospital outcomes of patients undergoing VT ablation from a large nationally representative sample of the United States population. Earlier studies have shown regional variations in outcomes after invasive cardiovascular procedures (1).
The patient was promptly admitted to the hospital for further evaluation. While the initial impression might not immediately suggest ventricular tachycardia (VT), a closer examination raises suspicion. An initial electrocardiogram (ECG) is provided below. What do you think? What is the rhythm? The rate is 132 bpm. What is the rhythm?
This was what was found: She had been at a different hospital less than a week ago at which time she had an an RCA stent for an lesion that had TIMI-3 flow. A Closer LOOK at the ECG in Figure-1: The ECG in Figure-1 shows sinus tachycardia — with QRS widening due to complete RBBB. What is the Lesson to be learned?
This immersive two-day event brought together renowned experts and cardiologists from different places, united in their pursuit of excellence in the management of supraventricular tachycardias (SVT). This distinguished faculty included Prof. Dr. Emin Evren Özcan , Prof. Dr. Barış Akdemir and Assoc.
Performance was best for pause (F 1 Score, 99%) and worst for paroxysmal supraventricular tachycardia (F 1 Score, 92%). for paroxysmal supraventricular tachycardia. We calculated classifier statistics for each arrhythmia, all arrhythmias and strips where the model identified normal sinus rhythm. for pause to 7.2%
He was admitted to the hospital for evaluation of these symptoms — but no ECG was done at that time. The conventional computer algorithm called “ sinus tachycardia, otherwise normal EKG ”. The rest of the patient’s hospital stay was uneventful and he was eventually discharged. The proximal LAD is now widely patent.
Electrical storm (ES) is associated with a high mortality, leads to recurrent hospitalization due to heart failure or ICD therapy deliveries. Ventricular tachycardia (VT) ablation has demonstrated efficacy in lowering VT recurrences but prompt ablation is challenging and the exact timing still unknown.
Let me tell you about her hospitalization, discharged 1 day prior, but it was at another hospital (I wish I had the ECG from that hospitalization): The patient is 40 years old and presented to another hospital with chest pain and SOB. The patient went into arrest pre-hospital. Junctional tachycardia? ).
BackgroundPregnancy increases the risk of supraventricular tachycardia (SVT) due to physiological changes. MethodsWe retrospectively analyzed 15 pregnant patients with SVT treated at Shenzhen Second People's Hospital ED from 2015 to 2023. This study reviews the management of SVT in pregnant patients in the emergency department (ED).MethodsWe
The rhythm is regular — at a rate just over 100/minute = sinus tachycardia ( ie, the R-R interval is just under 3 large boxes in duration ). Continuing with assessment of ECG #1 in Figure-2: The rhythm is sinus tachycardia at ~110/minute. Figure-2: I've labeled the initial ECG. The QRS complex is obviously wide.
Methods Data was collected retrospectively from the hospital medical records. The remaining 15% of patients presented with less common types of arrhythmias, including other supraventricular tachycardias (SVTs), retrograde dual atrioventricular nodal reentry, and premature ventricular contractions (PVC).
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? Troponins 34>33>43, likely secondary to myocardial injury from tachycardia. Reverted to atrial fibrillation with RVR while in the hospital 3 times and needed cardioversion. Sinus tachycardia does not go this fast.
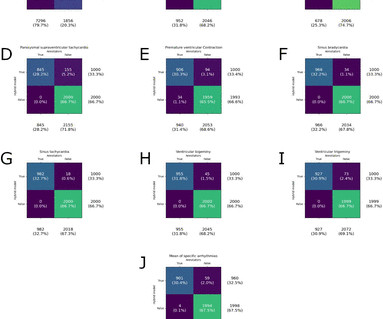
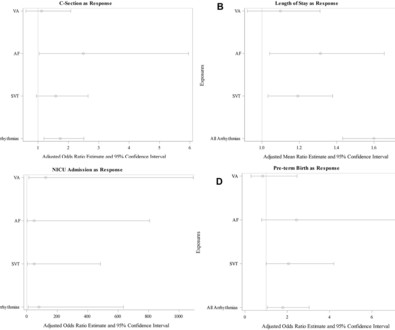
Methods This was a case–control study of women admitted in labour to one of eight hospitals of Northwell Health from January 2015 to June 2021. Objectives Examine the association between arrhythmias and adverse maternal outcomes in women with structurally normal hearts. Arrhythmia was previously diagnosed in 58.0% AF and 8.1%
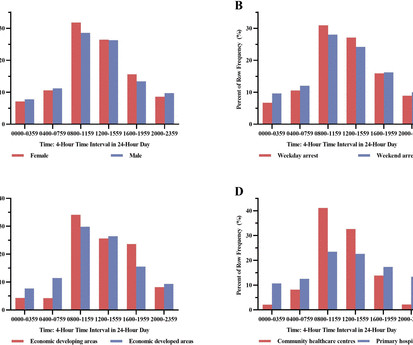
Background The circadian variation pattern of sudden cardiac arrest (SCA) occurred in Chinese community including both community healthcare centres and primary hospitals remains unknown. This study analysed the circadian variation of SCA in the Chinese community.
He was treated for infection and DKA and admission to hospital was planned. This is ischemic ST depression, and could be due to increasing tachycardia, with a heart rate over 130, but that is unlikely given that the patient is now complaining of crushing chest pain and that there was tachycardia all along.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content