This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
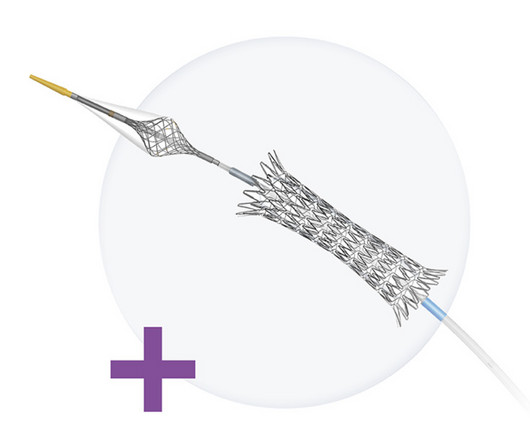
The Neuroguard Integrated Embolic Protection (IEP) system is an experimental treatment for carotid artery stenosis, also known as carotid artery disease, a condition in which fatty-waxy deposits known as plaque builds up and blocks the normal flow of blood in the large arteries on either side of the neck. Designed by Raleigh, N.C.-based
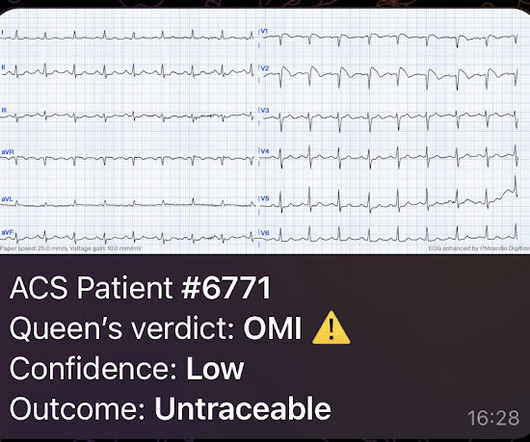
This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System. The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB.
Introduction:Medical therapy and endovascular therapy for intracranial atherosclerotic disease (ICAD) have evolved over the past two decades with improved medical therapy benchmarks, and improved techniques and patient selection for stenting. There were significantly higher incidences in uncontrolled hypertension (28.2%
Background:Postoperative complication rates of carotid endarterectomy (CEA) and carotid artery stenting (CAS) for carotid artery stenosis are recommended to be maintained below a certain threshold. Stroke, Volume 56, Issue Suppl_1 , Page ATP128-ATP128, February 1, 2025.
IntroductionVertebral artery stenting represents a viable option in treating symptomatic vertebral artery atherosclerotic stenosis. We included articles reporting patients > 18 years old with symptomatic extracranial vertebral artery stenoses due to atherosclerosis treated with stenting (with or without angioplasty).
BackgroundCarotid endarterectomy (CEA) is an established procedure for the treatment of extracranial internal carotid artery stenosis. Emergency CEA and carotid stenting procedures were excluded from the analysis. However, the type of anesthesia during elective CEA is still under debate.
Background:Persistent hypotension after carotid artery stenting (CAS) can lead to adverse outcomes, prolong length of stay (LOS), and increase hospital costs. A relation between decline of norepinephrine after stenting and persistent hypotension supports the role of catecholamine in BP control.
Background:Patients with atrial fibrillation were excluded from clinical trials evaluating carotid artery stent(CAS) or carotid endarterectomy (CEA).We Background:Patients with atrial fibrillation were excluded from clinical trials evaluating carotid artery stent(CAS) or carotid endarterectomy (CEA).We
I immediately looked for old charts, which were only available from another hospital, and an old echo confirmed inferior "akinesis" (which may also have persistent ST elevation). Angiogram: Widely patent RCA and LAD stents. Therefore, no stent was placed. (No He was treated with aspirin and heparin.
Anaphylaxis leads to plaque rupture or erosion leading to acute myocardial infarction (type II) and acute coronary stent thrombosis (type III). Case presentation A 47-year-old woman was admitted to the hospital due to an insect bite for 2 days and chest distress for more than 3 h. ng/ml(0–0.5 ng/ml).
She was admitted to the hospital with clinical signs of infection. The following day in the cath lab a borderline significant mid LAD stenosis was found. Decision was made to stent the lesion. ECG#4 (below) was recorded about one year after the hospital stay described above. The patient is a 60 something female.
Background:Carotid artery stenting (CAS) and carotid endarterectomy (CEA) are two types of carotid revascularization procedures performed on symptomatic patients. Frequently, carotid artery stenosis is found during stroke workup and these patients undergo revascularization during the same nonelective admission. vs 10.3%, P=0.582).
Or is it a very tight stenosis that does not allow enough flow to perfuse myocardium that has a high oxygen demand from severely elevated BP? So the patient was admitted to the hospital with no plan for an angiogram. This was a presumed culprit and a stent was placed. The ST depressions in I and aVL have resolved.
Here are other very interesting posts: Wellens' syndrome: to stent or not? Two ECG patterns were described by the original investigators in 1982 as being consistent with a Wellens’ Syndrome prediction of high-grade LAD stenosis. Total coronary occlusion, if very brief, may have minimal infarction and yet be very dangerous.
The red arrow shows a roughly 80% stenosis of the proximal LAD. The blue arrow shows another stenosis of the LAD distal to the first diagonal branch of about 99%. The green arrow shows a 95% stenosis of the ostium of the first diagonal branch. All three lesions had TIMI 2 flow prior to stenting.
He was admitted to the hospital for evaluation of these symptoms — but no ECG was done at that time. The red arrow points to a 90% stenosis in the proximal segment of the LAD. RAO Caudal View Post PCI This is the RAO Caudal view after thrombectomy and stent placement. An ECG was finally done at 9:17am on the 2nd hospital day.
However, CTA head and neck 4 days later demonstrated 90 percent stenosis of the mid left V2 at the C3‐4 level and a 75‐90 percent stenosis of the left mid V2 segment at the C5‐6 level (hard and soft plaque in these areas). He also had moderate stenosis of the right V4 segment.
Vascular surgeons at nearby hospitals had complained because they were seeing “a lot” of his patients having complications. Dormu performed an aortogram of the bilateral lower extremity with bilateral iliac runoff, which revealed a 90% stenosis of the right superficial femoral artery and 100% occlusion of all three tibial vessels.
years) underwent surgery for unruptured anterior communicating artery aneurysms in our hospital between January 2018 and January 2023.ResultsThe Coil embolization was performed for fifty‐four patients using various adjunctive techniques (simple, 7; double catheter, 15; balloon neck remodeling, 7; stent‐assisted, 26 (LVIS Jr.,
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. Angiography revealed a 30% nonobstructive stenosis of the mid LAD. Patient 1 remained in the hospital overnight. It was stented. This was a large OMI.
MRA head demonstrated multifocal arterial stenosis. Repeat CTA head/neck and CT perfusion showed severe stenosis of bilateral M1 segments and left greater than right A1 segments as well as ischemic penumbra in left ACA/MCA watershed territory. Her neurological exam improved to baseline on hospital day(HD) 9.On
Although he had a normal echocardiogram and stress test a year ago at a different hospital, due to his symptoms and intermediate-high risk probability of coronary artery disease (CAD), the decision was made to proceed with a cardiac catheterization using a trans-radial approach with a horizontal sweep technique.
CT angiography (CTA) showed near occlusive stenosis of the left carotid bulb with an acute thrombus within Supraclinoid Internal Carotid Artery (ICA) extending into the Left MCA and origin of Left Anterior Cerebral Artery (ACA). He underwent single pass complete recanalization, TICI 2C using Stent retriever and aspiration.
It was opened and stented. LM: No significant stenosis. LAD: luminal irregularities with a 40% stenosis at the take-off of a D3. D3 has a 95% tubular ostial stenosis. Culprit, stented) 3. LCX: Luminal irregularities, no significant stenosis. Two OM branches without significant stenosis. RCA: dominant.
Investigators assessed if empagliflozin could lower the risk of hospitalization for heart failure (HF) or death from cardiovascular disease (CVD). SMART 4 ( NCT04722250 ) studied patients with severe aortic stenosis and a small aortic annulus who underwent transcatheter aortic valve replacement (TAVR).
Patient underwent emergent mechanical thrombectomy with ADAPT to TICI3 revascularization with future plan for possible angioplasty and stenting of R vertebral stenosis. Subsequently admitted to neurocritical care unit and treated with dual antiplatelet therapy.
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chest pain that started while mowing the lawn. The LAD lesion was acute and required 3 stents to restore flow. Here is his ECG on arrival: What do you think?
The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis. What do you want to do now, considering you will need to awaken the hospital's only catheterization team, which must be alert for the next long day in the cath lab? Is it STEMI or NonSTEMI?
It was stented. Also, anterior MI could result from 1) ACS, but also from 2) severe ischemia due to combination of a hemodynamically significant LAD stenosis + severe hypotension during cardiac arrest. Current Emergency and Hospital Medicine Reports (2013) 1:4352. The troponin I peaked at 8.1. References : 1. J Electrocardiol.
Marked differences can be seen in the prevalence of coronary artery stenosis at autopsy by age and gender. In 30-39 year old women the rate of coronary stenosis at autopsy was 5/1,545 (0.3%) while 60-69 year old men had a prevalence of 12%, almost 40 times higher. The results of this dataset by age and gender follow.
There is ventricular hypertrophy in the absence of abnormal loading conditions, such as aortic stenosis, or hypertension, for example – of which the most common variant is Asymmetric Septal Hypertrophy. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital.
She was treated medically for NonSTEMI, pending next day cath, which showed ulcerated plaque and a 60% thrombotic stenosis in the LAD distal to the first diagonal. It was stented. For clarity — I've taken the chest leads from the 3 pre-hospital tracings in this case, and placed them side-by-side in Figure-1. Learning Points : 1.
61,62) The interventional community defines occlusive LM disease as >50% by FFR, or ≥75% stenosis,(63) but urgent or emergent intervention on lesions not meeting these thresholds is only imperative if it is a thrombotic lesion and the patient has refractory ischemic symptoms (i.e. TIMI 0/1 flow).(61,62) Knotts et al.
Case 4 Transient STEMI, serial ECGs prehospital to hospital, all troponins negative (less than 0.04 Angiogram showed a critical LAD thrombotic stenosis. The patient went to cath and had a distal LAD 99% stenosis with thrombus and TIMI-2 flow. It was stented. 100% LAD occlusion. He underwent CABG. Peak was 8.1
He was taken to the cath lab and underwent emergent intervention: Thrombotic stenosis of the proximal RCA (95% with evidence of plaque rupture) is the culprit for the patient's inferoposterior STEMI. He was successfully stented. The patient never arrested during his time at the hospital and his prognosis is good.
Kown, Asan Medical Center, Seoul, Korea Golden Bridge II Effect of an Artificial Intelligence-Based Clinical Decision Support System on Stroke Care Quality and Outcomes in Patients With Acute Ischemic Stroke : A Cluster-Randomized Clinical Trial: Zixiao Li, Beijing Tiantan Hospital, Capital Medical University, Beijing, China Friday, Feb.
Adult Cardiac Surgery Database Lead Author Title Publication Date Jacob Raphael Red Blood Cell Transfusion and Pulmonary Complications: The Society of Thoracic Surgeons Adult Cardiac Surgery Database Analysis The Annals of Thoracic Surgery January 2024 Joseph Sabik Multi-Arterial versus Single-Arterial Coronary Surgery: Ten Year Follow-up of One Million (..)
Institutional Coronary Artery Bypass Case Volumes and Outcomes European Journal of Heart Failure October 2023 Makoto Mori 1 Robotic Mitral Valve Repair for Degenerative Mitral Regurgitation The Annals of Thoracic Surgery August 2023 Carlos Diaz-Castrillion 2 Volume-Failure to Rescue Relationship in Acute Type A Aortic Dissections: An Analysis of The (..)
He works in a small hospital in Northern Michigan. The patient was transferred to a hospital with PCI capability. Here is the angiogram: Very tight stenosis in circumflex, but with TIMI-3 flow, thanks to thrombolytics. Here is the circumflex after stenting: Wide open The cardiologist called Dr. Lufkin back and said "Great call!!"
August 2024 Approvals Minima Stent System (P240003) (Approval Date: August 28, 2024) The Minima Stent System is an expandable cobalt-chromium metal mesh tube to reopen blood vessels in neonates, infants, and children with Coarctation of the Aorta and Pulmonary Artery Stenosis, specifically designed to expand as younger patients grow.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content