This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System. The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB.
The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI"). I advised that perhaps posterior leads would help to persuade the interventionalist, since the 2022 ACC recommendations include posterior STEMI as a formal STEMI equivalent, but only officially by 0.5
An ECG was recorded immediately at triage and, at this hospital, the Queen of Hearts is routinely used to determine cath lab activation. The door to balloon time was incredibly short and there was a 100% circumflex occlusion that was opened and stented. This patient had the onset of chest pain 24 hours before arrival to the ED.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. Cath lab was activated, and found a 95% proximal LAD occlusion which was stented. It’s unclear if the paramedic ECGs were seen or missed in the ED.
The cardiologist recognized that there were EKG changes, but did not take the patient for emergent catheterization because the EKG was “not meeting criteria for STEMI”. So the patient was admitted to the hospital with no plan for an angiogram. This was a presumed culprit and a stent was placed. Smith: What???!!!
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? This was stented. Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below).
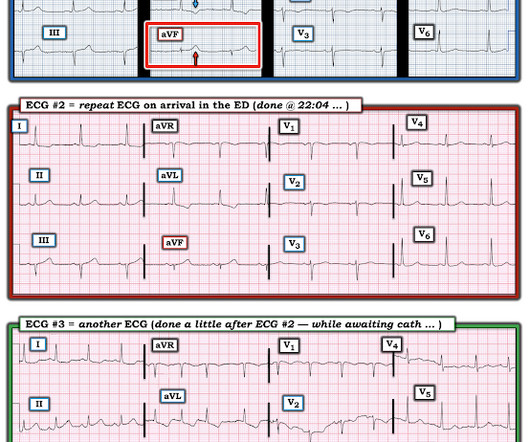
These tall T waves are associated with flattening ( straightening ) of the ST segment in the inferior leads — with slight S T elevation in leads V2-thru-V6 ( albeit not enough to qualify as a "STEMI" — Akbar et al, StatPearls, 2023 ). About 20 minutes later ( on the way to the hospital ) — the patient's CP resolved, and ECG #1 was recorded.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. The two cases were considered: Patient 1 was recognized by the ED provider and the cardiologist as having resolved “STEMI”. Patient 1 remained in the hospital overnight.
with ST elevated myocardial infarction (STEMI), 3.41% with unstable angina, 0.56% with stable angina, and 0.11% were diagnosed with various types of arrhythmias. SCAD-PCI revascularization frequently required three or more stents and had residual areas of dissection. Approximately 48.5% and 1.3%, respectively.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). As far as I can tell, there is only one randomized trial of immediate vs. delayed intervention for transient STEMI. Labs ordered but not yet drawn.
Intra-procedural data included access route, coronary anatomy, lesion complexity, number of stents deployed, door-to-balloon time for primary PCI, and any intra-procedural complications. and the average number of stents 2.6. The radial approach was used in 544/567 (95.94%), the average SYNTAX score was 34.8 ± 9.6,
These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). While this may be change that is reciprocal to an Acute/Subacute Inferior STEMI, the problem is that LV aneurysm may also manifest with this reciprocal change. In STEMI, they are generally upright and large in proportion to the QRS. This case is tough.
P.S.: Cardiac cath was performed — and showed a distal LA D "culprit" lesion that was successfully stented. It may look identical t o the ST-T wave appearance seen after a STEMI with marked troponin elevation, that has now reperfused ( be this reperfusion spontaneous — or by treatment with PCI or thrombolytics ).
He was admitted to the hospital for evaluation of these symptoms — but no ECG was done at that time. At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). RAO Caudal View Post PCI This is the RAO Caudal view after thrombectomy and stent placement.
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chest pain that started while mowing the lawn. There is a very small amount of STE in some of the anterior, lateral, and inferior leads which do NOT meet STEMI criteria.
Another ECG was recorded while awaiting the cath team: Now there is STEMI Let's look at that first (prehospital ECG) again: Very subtle! It was opened and stented. This was a weekend late evening, and so it took time the cath team to get in to the hospital. Peak trop was 7000 ng/L (since the intervention was so fast)!!
V5-6, is 97% specific for OMI! ) "The patient was transferred to cardiology at the referral hospital (we don't have cardiology in our hospital)." Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"."
However, upon entry into the respective hospital campus, the patient experienced restoration of pain and displayed an uncomfortable grimace. One stent was deployed with restorative TIMI-0 flow. it has been subsequently deemed a STEMI-equivalent. it has been subsequently deemed a STEMI-equivalent.
Data was collected from patients and their medical records during hospital stay using a structured data collection form. Types of ACS include stable angina 5.3% (n=8), unstable angina 24% (n=36), NSTEMI 28.7% (n=43), and STEMI 24% (n=36). All patients had interventional PCI with balloon and stent insertion.
The "criteria" for posterior STEMI are 0.5 Is it STEMI or NonSTEMI? What do you want to do now, considering you will need to awaken the hospital's only catheterization team, which must be alert for the next long day in the cath lab? The troponin I returned at 4.1 ng/mL (ULN = 0.030 ng/mL) , diagnostic of myocardial injury.
This was sent by : Jacob Smith, DO Emergency Medicine Resident Ohio Health Doctors Hospital Emergency Residency Christopher Lloyd, DO, FACEP Director of Clinical Education, USACS Midwest Case A 30 year old patient presents to triage with chest pain. This is diagnostic of inferior MI, though does not meet millimeter criteria for "STEMI."
Despite active CP — cath lab activation was deferred and this patient was transported to a local hospital without PCI capability. It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. Patient #1 in today's post did not get expert ECG interpretation.
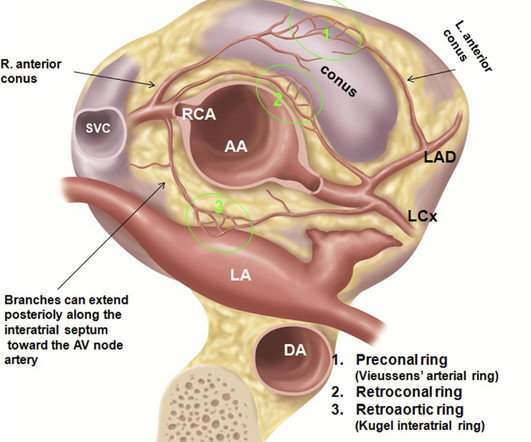
Wuhan Asia Heart Hospital, Wuhan, China Did you guess the diagnosis correctly? Final message Coronary arterial anomaly is a less discussed topic nowadays, unless & until, it intrudes an interventional cardiologist in his daily routine life, of delivering stents. We know, how adverse is the outcome of Left main STEMI.
He was treated for infection and DKA and admission to hospital was planned. 20% of cases that everyone would call a STEMI have a competely open artery by the time of angiogram 60-90 minutes later. While in the ED, patient developed acute dyspnea while at rest, initially not associated with chest pain.
According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician. A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. Here is the LAD after stent placement.
This morphology can be cause by or associated with cocaine: A Patient with Cocaine Chest Pain and Prehospital Computer interpretation of STEMI This is OMI of the anterior, lateral, and inferior walls until proven otherwise. But it does not meet STEMI criteria and it was not initially recognized. The cath lab was now activated.
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. No appreciable skin pallor. Is this OMI?
The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Similarly, STEMI guidelines call for urgent angiography for refractory ischemia or electrical/hemodynamic instability, regardless of ECG findings. So the RCA was stented. Vitals were HR 58 BP 167/70 R20 sat 96%.
It was opened and stented. Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Therefore it is not a STEMI. But what we truly care about is coronary occlusion, for which STEMI is just a surrogate that is only about 75% sensitive for occlusion. RCA: dominant.
This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. He did, found the true culprit, and went back in to stent it. Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI.
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. It was stented. If you want to understand aVR, read this.]
This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. When OMI is captured in this early phase, there exists the highest amount of salvageable myocardium and least likelihood of heart failure at hospital discharge. A mid-LAD culprit lesion was identified and stented.
He had been seen several weeks ago at an outside hospital for a similar issue and had been discharged home, presumably after unremarkable workup. He was successfully treated with one drug eluting stent. He was ultimately discharged after a brief, uncomplicated hospital course. Occurred while driving to a doctor’s appointment.
There is an obvious inferior STEMI, but what else? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. This STE is diagnostic of Right Ventricular STEMI (RV MI). In fact, the STE is widespread, mimicking an anterior STEMI. He was successfully stented.
These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? Appropriately, the physicians repeated the ECG 20 minutes later and it was diagnostic of anterior STEMI. QTc is the computer measurement. 100% LAD occlusion.
EMS recorded these prehospital ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 She was having a transient STEMI, briefly. It did not progress to full STEMI with loss of the anterior wall, as in this case. It was stented. She called 911. Learning Points : 1. See this case.
It was treated with and dual "kissing balloons" and drug eluting stents. Here is the post stent ECG: There is greater than 50% resolution of ST elevation (all but diagnostic of successful reperfusion) and Terminal T-wave inversion (also highly suggestive of successful reperfusion). TIMI flow is 0. Door to balloon time was 51 minutes.
He reported a history of ischemic cardiomyopathy with coronary stent placement approximately 10 years prior, but could not recall the specific artery involved. He requested transport to the hospital out of an abundance of caution, and all subsequent serial ECG’s showed no changes from Figure 1-2, shown above. Attached is the first ECG.
In the context of the abnormal ST elevation we see in leads III and aVF I interpreted this mirror-image J-point depression as a reciprocal change in this LBBB patient whose ECG is diagnostic of an acute inferior STEMI. The Case Continues: The initial ECG was transmitted to the ED physician at the hospital.
There is STE that does not meet STEMI criteria in V1-V6. Troponin profile The patient underwent angiography and had a 90% thrombotic proximal LAD lesion that was stented. I focus my attention on the first 2 ECGs, both of which were done prior to arrival in the hospital. Precordial leads: What do you think?
His initial cTnI at the receiving hospital was 27 ng/mL, and no further troponins were measured thereafter. Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent. The patient’s ECG on arrival at the emergency department is shown below. To our knowledge, the patient did well.
Post by Smith, with short article by Angie Lobo ( [link] ), a third year intermal medicine resident at Abbott Northwestern Hospital Case A 30-something woman with no past history, who is very fit and athletic, presented with 1.5 It is equivalent to a transient STEMI. The lesion was stented. hours of substernal chest pressure.
Admitted to the hospital service for further evaluation and management." Diagnosis: Acute non-ST segment elevation MI (Non-STEMI, or NSTEMI) Second troponin returned at around 0200: 15,894 ng/L 0245 (unclear if ongoing pain or not) Inferoposterior (and lateral V5-6) reperfusion findings. No further ECG were ever recorded.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















































Let's personalize your content