This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Pendell Meyers I received this prehospital ECG (we receive prehospital ECGs by telemetry from EMS in a large area around our hospital) and was told that there was a patient in her 50s with chest pain who was headed to an outside hospital (which happens to be a catheterization center). Here is the ECG: What do you think?
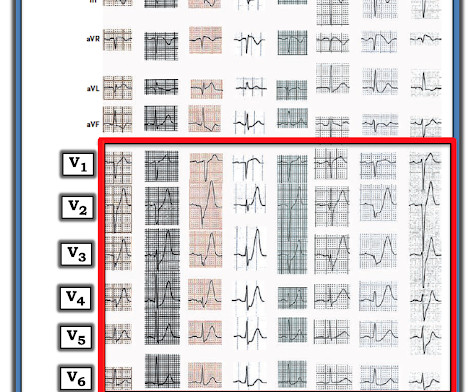
This is a 45 yo male who had an inferior STEMI 6 months prior, was found to have severe LAD and left main disease, and was supposed to be set up for CABG a few weeks later, but did not follow up. But it could be anterior STEMI. 40% of anterior STEMI has upward concavity in all of leads V2-V6. is likely anterior STEMI).
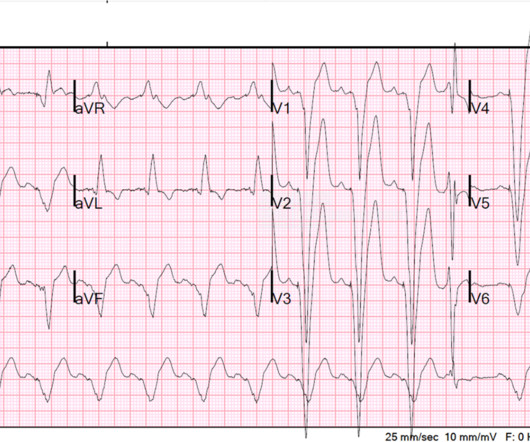
BUT — Cardiac catheterization done a little later did not reveal any significant stenosis. Despite the absence of significant coronary stenosis on her post-arrest cath — the ECG in Figure-1 is clearly diagnostic of an extensive anterolateral STEMI ( presumably from acute LAD [ L eft A nterior D escending ] coronary artery occlusion).
The cardiologist recognized that there were EKG changes, but did not take the patient for emergent catheterization because the EKG was “not meeting criteria for STEMI”. Or is it a very tight stenosis that does not allow enough flow to perfuse myocardium that has a high oxygen demand from severely elevated BP? Smith: What???!!!
This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System. The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB.
Even in patients whose moderate stenosis undergoes thrombosis, most angiograms show greater than 50% stenosis after the event. However, one can certainly imagine that many thromboses of non-obstructive lesions completely lyse and do not leave a stenosis on same day or next day angiogram. From Gue at al.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). As far as I can tell, there is only one randomized trial of immediate vs. delayed intervention for transient STEMI. Labs ordered but not yet drawn.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. The two cases were considered: Patient 1 was recognized by the ED provider and the cardiologist as having resolved “STEMI”. Patient 1 remained in the hospital overnight.
is very specific for STEMI , and there is some evidence, as well as rationale, that a paced rhythm behaves similarly. Here is one case of anterior STEMI in a paced rhythm. Here is a case of lateral STEMI in a paced rhythm. LV Ejection Fraction at the time of this hospitalization was 10%.
The estimated left ventricular ejection fraction is 58 % Aortic stenosis, mild, 9.0 We found that 38% of out of hospital ventricular fibrillation was due to STEMI. The patient thus did not need immediate angiography. An echocardiogram showed: Left ventricular hypertrophy concentric. mmHg mean gradient. cm^2 valve area.
The culprit lesion was a complex calcified mid LAD stenosis involving the first and second diagonal branches. Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). The case doesn't come up for quality assurance because that is only done for STEMI patients.
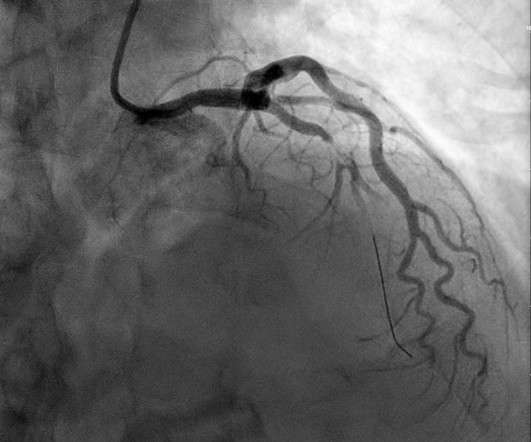
He was admitted to the hospital for evaluation of these symptoms — but no ECG was done at that time. At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). The red arrow points to a 90% stenosis in the proximal segment of the LAD. RAO Caudal view: This is the RAO Caudal view.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? His response: “subendocardial ischemia.
Another ECG was recorded 5 minutes later just before arrival at the hospital: Similar The patient was transported to a nearby suburban hospital with PCI capabilities while my partner cared for her. These findings are diagnostic of an apical OMI as a result of LAD Occlusion. She was defibrillated and resuscitated. Learning Points: 1.
The "criteria" for posterior STEMI are 0.5 Is it STEMI or NonSTEMI? The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis. The troponin I returned at 4.1 ng/mL (ULN = 0.030 ng/mL) , diagnostic of myocardial injury. mm STE in one lead.
Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Therefore it is not a STEMI. But what we truly care about is coronary occlusion, for which STEMI is just a surrogate that is only about 75% sensitive for occlusion. Some are STEMI-equivalents. RCA: dominant.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. A transthoracic echocardiogram showed an LV EF of less than 15%, critically severe aortic stenosis , severe LVH , and a small LV cavity. Look at the aortic outflow tract. What do you see?
This meets "STEMI criteria" However, there is very high voltage, with a very deep S-wave in V2 and tall R-wave in V4. The morphology is not right for STEMI. My interpretation: LVH with secondary ST-T abnormalities, exaggerated by stress, not a STEMI. This is very good evidence that the ST elevation is not due to STEMI.
Cath at approximately 0945: "The LAD had a 90% proximal stenosis with TIMI 3 flow which corresponds to his ECG although LV function remains preserved. With nitroglycerin there is improvement in the 90% stenosis but still persistent stenosis consistent with the dynamic nature of his presentation. When is it anterior STEMI?
There is clearly sufficient STE for STEMI criteria in leads V2 and aVL, but lead I has less than 1.0 mm of STE - thus, technically this ECG does not meet STEMI criteria, although it is a quite obvious OMI. This ECG was immediatel y discussed with the on-call cardiologist who said the ECG was "concerning but not a STEMI."
The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Current Emergency and Hospital Medicine Reports (2013) 1:4352.
There is ventricular hypertrophy in the absence of abnormal loading conditions, such as aortic stenosis, or hypertension, for example – of which the most common variant is Asymmetric Septal Hypertrophy. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital.
These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? Appropriately, the physicians repeated the ECG 20 minutes later and it was diagnostic of anterior STEMI. Angiogram showed a critical LAD thrombotic stenosis.
EMS recorded these prehospital ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 She was having a transient STEMI, briefly. It did not progress to full STEMI with loss of the anterior wall, as in this case. Patients with transient occlusion may manifest only transient STEMI on ECG.
90% stenosis of the proximal ramus intermedius, pre procedure TIMI II flow The ramus intermedius is a normal variant on coronary anatomy that arises between the LAD and LCX. The patient was started on dual antiplatelet therapy and discharged from the hospital on day 3 without further event.
I sent this ECG to the Queen of Hearts (PMcardio OMI), and here is the verdict: You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form Then I learned that a Code STEMI was activated for concern of anterior "STEMI" in V1-V2. High sensitivity troponin I was 23 ng/L.
First high sensitivity troponin I = 4 ng/L (nearly below the limit of detection) Angiogram: --Culprit is 99 % stenosis in the proximal ostial LAD --LCX is a large OM with a large lateral segment, the lateral segement has a diffuse 90% disease in the ostial proximal segment of it. This is FAR LESS than all other studies of shockable arrest.
Angiogram around 9am: Culprit lesion mid LAD 100% stenosis TIMI 0 TIMI 3 after PCI Severe apical dyskinesis, severe anteroapical akinesis. Once in a while they die during the hospitalization, but I fear that many more like this patient survive for now to develop lifelong increased morbidity and mortality from heart failure.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. Angiography : LMCA — 90-99% osteal stenosis. LCx — 50-69% stenosis of the 1st marginal branch; with 100% distal LCx occlusion. The patient was extubated on Day-3 of the hospital stay. The below ECG was recorded. RCA — 100% proximal occlussion.
There is an obvious inferior STEMI, but what else? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. This STE is diagnostic of Right Ventricular STEMI (RV MI). In fact, the STE is widespread, mimicking an anterior STEMI. EKG is pictured below: What do you think?
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chest pain that started while mowing the lawn. There is a very small amount of STE in some of the anterior, lateral, and inferior leads which do NOT meet STEMI criteria.
But limitation of this ST elevation to a single lead is not consistent with any distribution of a STEMI. Apparently while waiting on the hospital floor for the decision regarding optimal aortic replacement — the patient took one of his sublingual NTG ( nitroglycerin ) tablets. Cardiac Cath showed patent coronary arteries!
He works in a small hospital in Northern Michigan. But it does not meet the ridiculous "STEMI criteria" since there is not 1 mm of STE in any lead. The patient was transferred to a hospital with PCI capability. Here is the angiogram: Very tight stenosis in circumflex, but with TIMI-3 flow, thanks to thrombolytics.
Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. An EKG from a year prior was available for comparison: The ED physician noted Initial EKG here read by the computer as a STEMI, however, there is a very poor baseline and a lot of artifact. See reference and discussion below.
They recorded this ECG: Obvious inferior STEMI/OMI What else? The EMS ECGs: As per Dr. Smith the diagnosis of acute inferior STEMI is obvious from the history of new, severe CP in a patient with the initial EMS ECG that I show below ( TOP tracing in Figure-1 ). He called 911. Medics recorded a BP of 79/52 with pulse of 47.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content