This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
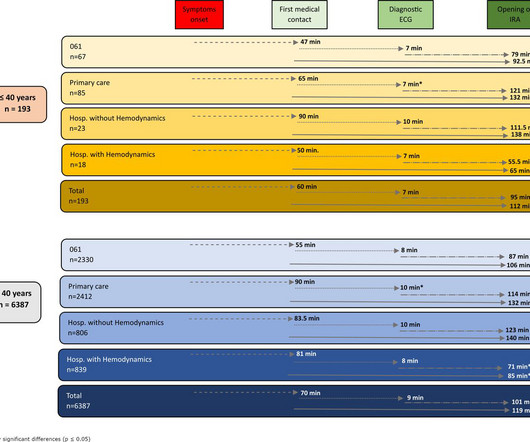
Introduction ST-elevation myocardial infarction (STEMI) is one of the most prevalent presentations in young patients. Methods A retrospective, multicentre cohort study was carried out in 6799 patients diagnosed with STEMI. to 2.06) (p<0.001) or going to a hospital without haemodynamics (RR 1.55, 95% CI 1.45
This narrative review aims to evaluate strategies for reducing door-to-balloon (D2B) time in ST-elevation myocardial infarction (STEMI) patients, focusing on pre-hospital, in-hospital, and technological innovations, as well as addressing challenges to ensure sustainability.
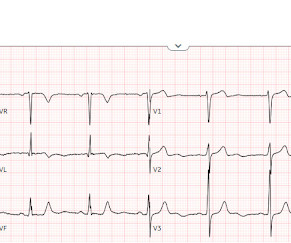
Written by Pendell Meyers I received this prehospital ECG (we receive prehospital ECGs by telemetry from EMS in a large area around our hospital) and was told that there was a patient in her 50s with chest pain who was headed to an outside hospital (which happens to be a catheterization center). Here is the ECG: What do you think?
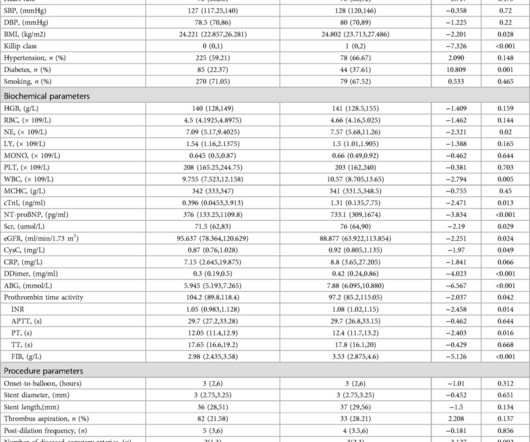
However, whether immediate blood glucose and FIB levels affect coronary blood flow during primary percutaneous coronary intervention (PCI) remains unclear.ObjectiveTo explore the correlation between admission blood glucose (ABG), fibrinogen (FIB) and slow blood flow during primary PCI for acute ST segment elevation myocardial infarction (STEMI).MethodsA
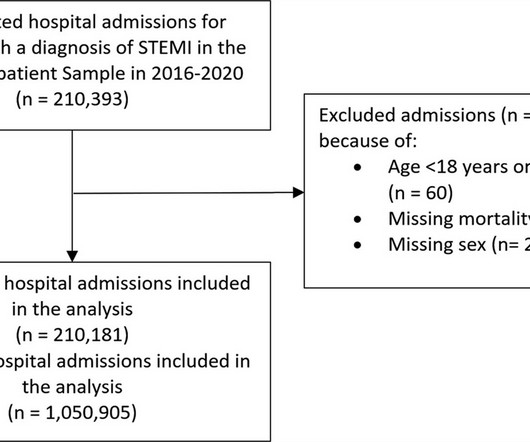
Background It is unclear how COVID-19 pandemic affected care and outcomes among patients who are diagnosed with ST-elevation myocardial infarction (STEMI) in the USA. Results There were 1 050 905 hospitalizations with STEMI, and there was an 8.2% Results There were 1 050 905 hospitalizations with STEMI, and there was an 8.2%
Microvascular resistance reserve (MRR) measured directly after primary PCI was an independent predictor of all-cause mortality or hospitalization for heart failure (HF) in patients with a STEMI over long-term follow-up, according to the results of a pooled analysis.
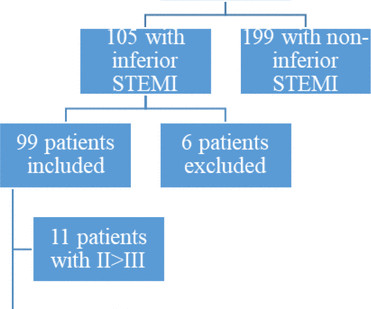
Background ST elevation myocardial infarction (STEMI) represents a cardiac emergency. Inferior STEMI represents a dilemma for cardiologists. Methods We performed a single-centre retrospective cohort analysis of all patients admitted to our hospital from 2008 to 2020 with a diagnosis of inferior STEMI.
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? This is the response he got: Interventionist: "No STEMI, no cath. After stabilizing the patient and recording more ECGs, he tried again: Interventionalist: "It isn't a STEMI." It is a STEMI equivalent. We don't know how many though.
This is a 45 yo male who had an inferior STEMI 6 months prior, was found to have severe LAD and left main disease, and was supposed to be set up for CABG a few weeks later, but did not follow up. But it could be anterior STEMI. 40% of anterior STEMI has upward concavity in all of leads V2-V6. is likely anterior STEMI).
See these 2 articles Association between pre-hospital chest pain severity and myocardial injury in ST elevation myocardial infarction: A post-hoc analysis of the AVOID study Author links open overlay panel [link] 1 Background We sought to determine if an association exists between prehospital chest pain severity and markers of myocardial injury.
In fact, it read: ** **ACUTE MI / STEMI ** ** The physicians caring for the patient activated the cath lab for "STEMI". The interventionalist and cath team came to the hospital, and when the interventionalist saw the ECG, he inquired further and elicited a family history of Brugada syndrome. And it is clearly Brugada phenotype.
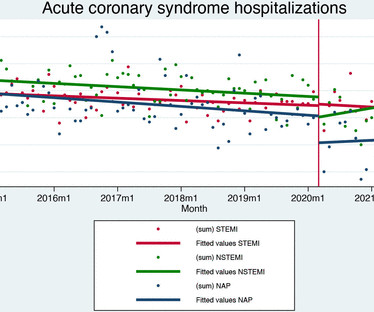
Aims We evaluated the effects of the COVID-19 pandemic on hospital admission and quality of care for acute coronary syndrome. Data on 21 001 patients were included (7057 ST-elevation myocardial infarction (STEMI), 7649 non-ST elevation myocardial infarction (NSTEMI) and 6295 unstable angina).
The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI"). I advised that perhaps posterior leads would help to persuade the interventionalist, since the 2022 ACC recommendations include posterior STEMI as a formal STEMI equivalent, but only officially by 0.5
Jason was very skeptical of STEMI. This also argues against STEMI. Unfortunately, this option might not be available for pre-hospital tracings ( but it can be done once the patient arrives in the ED for their initial hospital tracing ). He complained of 3 days of diarrhea and abdominal pain. What do you think?
He has now implemented the Queen of Hearts in his hospital. The emergency physician asked the advice of Dr. Reiters because of absence of STEMI criteria. This case was sent by Dr. Jean-christophe Reiters, an interventionalist in Belgium. He has been following the blog for 4 years. He wanted to share one of the first cases.
Both microvascular resistance reserve and index of microcirculatory resistance were shown to be independent predictors for the composite of all-cause mortality or hospitalization for heart failure [2]. Immediate Microvascular Physiology After Mechanical Coronary Reperfusion of STEMI. J Am Coll Cardiol. 2024 May, 83 (21) 2077–2079.
Background:Little is known about the clinical relevance of interleukin (IL)-6 and the severity of patients with acute ST-elevation myocardial infarction (STEMI). This study examined the possible associations of plasma IL-6 concentrations with TIMI scores in STEMI patients treated with primary percutaneous coronary intervention (PCI).Methods:The
An ECG was recorded immediately at triage and, at this hospital, the Queen of Hearts is routinely used to determine cath lab activation. The Non-STEMI, which was an OMI, was diagnosed much faster with AI on the ECG than with troponin. This patient had the onset of chest pain 24 hours before arrival to the ED.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. This case is an example of the steps we can all take in daily practice as the paradigm shifts from STEMI to OMI.
BackgroundThere may be variability in willingness to perform percutaneous coronary intervention (PCI) in higherrisk patients who present with STsegmentelevation myocardial infarction (STEMI). We compared patientlevel characteristics of patients who did and did not undergo PCI at each hospital. versus 7.4%,P<0.001), versus 5.1%,P<0.001)
About 20 minutes later ( on the way to the hospital ) — the patient's CP resolved, and ECG #1 was recorded. mmm ECG Blog #193 — Reviews the concept of why the term “OMI” ( = O cclusion-based MI ) should replace the more familiar term STEMI — and — reviews the basics on how to predict the " culprit " artery.
The most recent study found a NPV of 100% of triage ECGs labeled ‘normal’ or ‘otherwise normal’ for final hospital diagnosis of ACS, and concluded that avoiding physician interruption would “alleviate interruptions in workflow and improve patient safety.” Cath lab was activated, with door-to-cath time of 118 minutes.
The cardiologist recognized that there were EKG changes, but did not take the patient for emergent catheterization because the EKG was “not meeting criteria for STEMI”. So the patient was admitted to the hospital with no plan for an angiogram. Most STEMI have peak troponin I over 1000 ng/L and most NSTEMI below that level.
Background Despite advances in percutaneous coronary intervention (PCI) for ST segment elevation myocardial infarction (STEMI), in-hospital mortality remains a concern, highlighting the need for the identification of additional risk factors such as serum iron levels. μmol/L) and a control group (Fe ≥7.8 μmol/L).
Background The diagnosis of a left ventricular (LV) thrombus in patients with ST-segment elevation myocardial infarction (STEMI) remains challenging. Methods We retrospectively evaluated 337 consecutive STEMI patients. All patients underwent transthoracic echocardiography (TTE) and CMRI during their index hospitalization.
This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System. The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB.
Prompt cath is therefore advised if the post-ROSC shows an acute STEMI. To Emphasize: The phenomenon of T-QRS-D is not needed in today's case to recognize the acute STEMI. Retrospective questioning of the driver who brought this patient to the hospital revealed that he was having chest pain as the reason for presenting to the ED.
Despite the absence of significant coronary stenosis on her post-arrest cath — the ECG in Figure-1 is clearly diagnostic of an extensive anterolateral STEMI ( presumably from acute LAD [ L eft A nterior D escending ] coronary artery occlusion). The rhythm in ECG #1 is regular and supraventricular at a rate of ~75/minute.
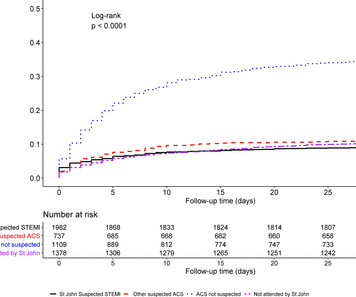
Background Early recognition of ST-segment elevation myocardial infarction (STEMI) is needed for timely cardiac monitoring and reperfusion therapy. The national cardiac (ANZACS-QI) registry and national administrative datasets capture all New Zealand public hospital admission diagnoses and mortality data.
These tall T waves are associated with flattening ( straightening ) of the ST segment in the inferior leads — with slight S T elevation in leads V2-thru-V6 ( albeit not enough to qualify as a "STEMI" — Akbar et al, StatPearls, 2023 ). About 20 minutes later ( on the way to the hospital ) — the patient's CP resolved, and ECG #1 was recorded.
The Society of Cardiovascular Angiography and Interventions has published an expert consensus statement on the management of patients with ST-elevation myocardial infarction.
Is primary PCI superior to thrombolysis in the first hour of STEMI ? No, it is not. I know, most interventional cardiologists cannot accept this fact and would strongly disagree. Still, they know very well there is no clear data to back up their belief. Read ref 1, 2. Reference 1.
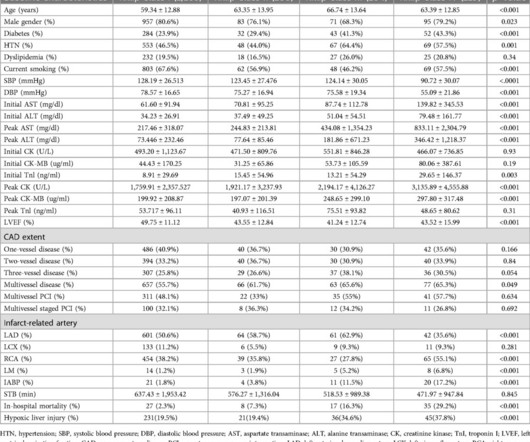
IntroductionHypoxic liver injury (HLI) and Killip classification are poor prognostic factors in patients with ST-segment elevation myocardial infarction (STEMI). In-hospital mortality was directly related to Killip classification (2.3%, 7.3%, 16.3%, 29.2%) with statistical significance.
Patients were categorized as frail if they had a hospital frailty risk score (HFRS) of 5 or higher, and non-frail if their score was below 5. Patients were categorized as frail if they had a hospital frailty risk score (HFRS) of 5 or higher, and non-frail if their score was below 5. 10.82), GI hemorrhage (AOR = 2.03, 95% CI: 1.63-2.53),
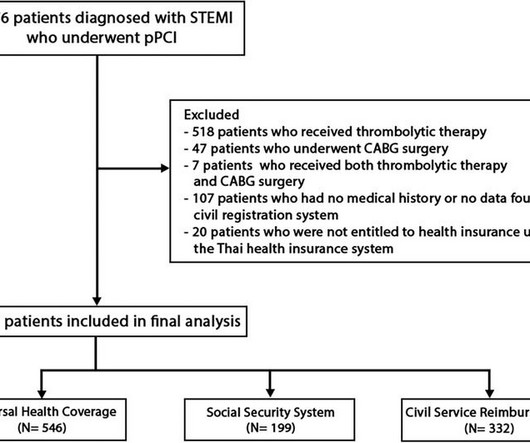
BackgroundIn Thailand, access to specific pharmaceuticals and medical devices for ST-elevation myocardial infarction (STEMI) patients is restricted within certain healthcare systems, leading to inequalities in the quality of medical care among different healthcare systems.
BackgroundThe pharmacoinvasive (PhI) strategy is the standard-of-care for ST-elevation myocardial infarction (STEMI) patients when primary percutaneous coronary intervention (pPCI) is unfeasible. Optimal timing for post-fibrinolytic PCI (lysis-PCI) remains elusive.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS.
STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al. Circulation. 2017;135(16):1490–3.
She presented to an outside hospital after several days of malaise and feeling unwell. It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI. At the time of admission, her vital signs were normal. Heart rate was in the 80s.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. The patient had a protracted hospitalization and did not survive.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. The two cases were considered: Patient 1 was recognized by the ED provider and the cardiologist as having resolved “STEMI”. Patient 1 remained in the hospital overnight.
Inferior STEMI without inferior ST elevation. The development of an inferior-posterior STEMI, from prehospital to hospital Case 6. Is this STEMI? Subtle Inferoposterolateral STEMI Details in every case make it even better, so click on the link!! Chest Pain in a 61 year old male. Inferior Hyperacute T-waves Case 3.
Although there are more criteria to consider when looking for OMIs compared to STEMIs, anyone can learn them, and this guide is intended to help accelerate that process! The guide organizes OMIs into categories based on each of the steps outlined by Drs. I’ve accessed this hand OMI Pocket Guide on both my ipad and iphone.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content