This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
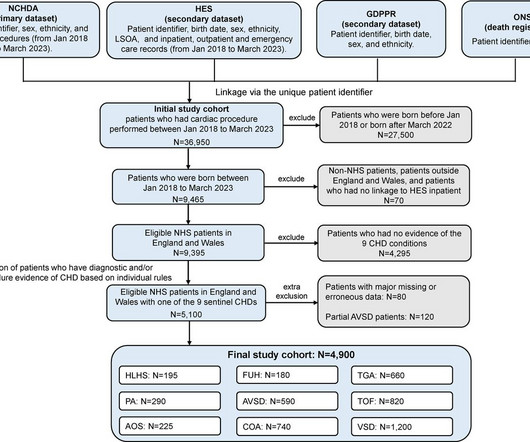
The outcomes of cardiac intervention timing, infant mortality and hospital care utilisation, were described by birth eras, and riskfactors were explored using multivariable regression. Compared with prepandemic, there was no evidence for delay in treatment procedures in transition, restrictions or postrestrictions eras.
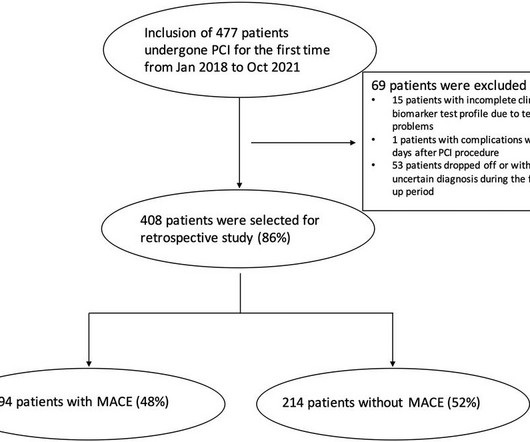
Percutaneous coronary intervention (PCI), as a relatively rapid and effective minimally invasive treatment for coronary heart disease (CHD), can effectively relieve coronary artery stenosis and restore myocardial perfusion. However, the occurrence of major adverse cardiovascular events (MACE) is a significant challenge for post PCI care.
Background:The uneven distribution of intracranial atherosclerotic stenosis (ICAS) along the internal carotid artery (ICA) had been described in early clinicopathological studies, yet related, large-scale data is lack despite the widespread utilization of angiography.
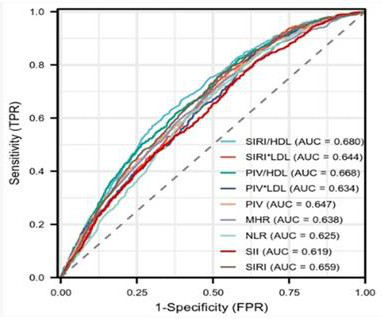
This study aimed to investigate the association between various complex indexes of blood cell types and lipid levels with the severity of coronary artery stenosis and their predictive value in coronary heart disease (CHD). Results It revealed a positive correlation between all complex indexes and the severity of coronary artery stenosis.
Or is it a very tight stenosis that does not allow enough flow to perfuse myocardium that has a high oxygen demand from severely elevated BP? However, in light of riskfactors for atherosclerotic disease and dynamic EKG changes today, we will pursue a CTCA tomorrow for further evaluation of coronaries. Smith: What???!!!
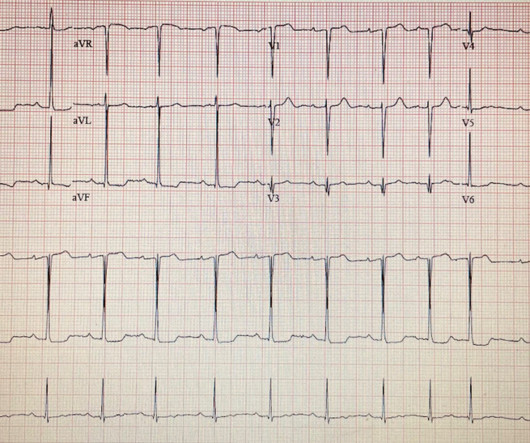
BUT — Cardiac catheterization done a little later did not reveal any significant stenosis. Despite the absence of significant coronary stenosis on her post-arrest cath — the ECG in Figure-1 is clearly diagnostic of an extensive anterolateral STEMI ( presumably from acute LAD [ L eft A nterior D escending ] coronary artery occlusion).
Although low BP can be seen in those hospitalized with signs of shock, the most common scenario involves non-severe, asymptomatic hypotension in patients receiving foundational therapy for HFrEF, where premature down-titration or discontinuation of GDMT should be avoided.
Background:The optimal treatment in patients with severe aortic stenosis (AS) and small aortic annulus (SAA) remains to be determined. Circulation, Ahead of Print.
Atrial Fibrillation 2. Cardiomyopathy with mural thrombus 3. Patent Foramen Ovale 4. Severe calcific Aortic (valve) Stenosis 5. Mechanical prosthetic valve Severe carotid artery stenosis is also implicated in embolic stroke. The following link provides a robust, and comprehensive, review of this entity.
Even in patients whose moderate stenosis undergoes thrombosis, most angiograms show greater than 50% stenosis after the event. However, one can certainly imagine that many thromboses of non-obstructive lesions completely lyse and do not leave a stenosis on same day or next day angiogram.
1 Low/zero fluoroscopy safety was evaluated further by a secondary analysis of data from electronic health records from 45 hospitals within the Mercy Health integrated hospital network, comparing PAEs between procedures with low fluoroscopy (two minutes or fewer) versus conventional fluoroscopy (three minutes or longer).1
This study aims to validate T max delay and mismatch as predictors of 30-day ischemic stroke recurrence.Methods:This is a single-center study from a comprehensive stroke center including hospitalized patients with symptomatic intracranial arterial stenosis (50-99%) of the intracranial ICA and proximal middle cerebral artery (M1 or proximal M2).
I quickly reviewed the patient’s records and saw that she was a 53 year old woman with a history of BMI 40, but no other identifiable riskfactors for coronary artery disease. On hospital day 3, the patient had recurrence of symptoms and the following EKG was obtained. "A patient just arrived as a transfer for NSTEMI."
He was admitted to the hospital for evaluation of these symptoms — but no ECG was done at that time. The red arrow points to a 90% stenosis in the proximal segment of the LAD. The rest of the patient’s hospital stay was uneventful and he was eventually discharged. An ECG was finally done at 9:17am on the 2nd hospital day.
However, CTA head and neck 4 days later demonstrated 90 percent stenosis of the mid left V2 at the C3‐4 level and a 75‐90 percent stenosis of the left mid V2 segment at the C5‐6 level (hard and soft plaque in these areas). He also had moderate stenosis of the right V4 segment.
Background:Myocardial infarction with nonobstructive coronary artery disease (MINOCA) is a special syndrome with clear evidence of myocardial ischemia, but no clear stenosis of coronary artery imaging sign. Circulation, Volume 150, Issue Suppl_1 , Page A4143007-A4143007, November 12, 2024.
Given the consistency of the clinical profile with typical angina, associated riskfactors, and abnormal ECG findings, a cardiology consult was promptly requested. Aortic Stenosis f. Left Main stenosis (not thrombosed) c. Aortic Stenosis [No Hx syncope, and no systolic murmur] f. This results in Type I MI.
A completely healthy 30-something year old woman with no cardiac riskfactors had sudden onset of bilateral trapezius pain that radiated around to her throat. R Riskfactors = 0 5. Risk of 30-day adverse events is less than 1.7%. The ECG told the story. The first troponin was below the level of detection (LoD).
mg tablet), ananti-inflammatory atheroprotective cardiovascular treatment, to reduce the risk of myocardial infarction (MI), stroke, coronary revascularization, and cardiovascular death in adult patients with established atherosclerotic disease or with multiple riskfactors for cardiovascular disease.
At 3 and 6 months after ablation in patients with paroxysmal and non-paroxysmal AF, researchers did not observe any reported deaths or certain serious complications, including coronary spasm, persistent phrenic nerve palsy, atrio-esophageal fistula, or pulmonary vein stenosis. Lucas Boersma , electrophysiologist, St. doi:10.1001/jama.285.18.2370
Levine Professor of Medicine at Harvard Medical School , former chair of the department of medicine and physician-in-chief emeritus at Brigham and Women’s Hospital in Boston; Daniel J. While some genes have been associated with the risk of developing AAA disease, none is thought to cause an AAA by itself. Rader , M.D.,
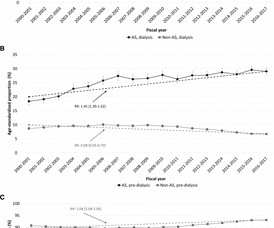
Objective To investigate temporal trends of chronic kidney disease (CKD) among patients with incident aortic stenosis (AS) and to compare these trends with that of a matched control population. The predialysis subgroup had at least one hospital or two billing diagnostic codes of CKD. Three subgroups were considered.
mg tablet), ananti-inflammatory atheroprotective cardiovascular treatment, to reduce the risk of myocardial infarction (MI), stroke, coronary revascularization, and cardiovascular death in adult patients with established atherosclerotic disease or with multiple riskfactors for cardiovascular disease.
This study aimed to confirm the prognostic value of a novel angiographic microvascular resistance (AMR) index in patients undergoing transcatheter aortic valve replacement.Methods and ResultsWe prospectively included 335 patients with severe aortic stenosis who underwent transcatheter aortic valve replacement at Fuwai Hospital.
More than 8 million Americans visit hospital emergency departments experiencing chest pain every year. Coronary computed tomography angiography (CCTA) is routinely used to diagnose CAD caused by the narrowing (stenosis) or blockage of the coronary arteries that supply the heart with blood. mg tablets.”
Background:The secondary prevention of symptomatic intracranial atherosclerotic stenosis (sICAS) remains a significant challenge. In addition, coronary heart disease (adjusted HR=1.674, 95% CI: 1.013-2.766, P=0.044) was identified as a riskfactor associated with composite outcome during the 1-year follow-up.
Marked differences can be seen in the prevalence of coronary artery stenosis at autopsy by age and gender. In 30-39 year old women the rate of coronary stenosis at autopsy was 5/1,545 (0.3%) while 60-69 year old men had a prevalence of 12%, almost 40 times higher. The results of this dataset by age and gender follow.
Meschia is a pioneer in the study of inherited riskfactors for ischemic stroke and has had a longstanding commitment to providing the latest evidence for carotid revascularization as a means for stroke prevention. Meschia’s lecture, “Asymptomatic Carotid Stenosis: Current and Future Considerations,” will be presented Feb.
Part 2: Empirical Studies in Cardiac Surgery; Risk Model Recommendations The Annals of Thoracic Surgery January 2022 David Shahian Social RiskFactors in Society of Thoracic Surgeons Risk Models.
Institutional Coronary Artery Bypass Case Volumes and Outcomes European Journal of Heart Failure October 2023 Makoto Mori 1 Robotic Mitral Valve Repair for Degenerative Mitral Regurgitation The Annals of Thoracic Surgery August 2023 Carlos Diaz-Castrillion 2 Volume-Failure to Rescue Relationship in Acute Type A Aortic Dissections: An Analysis of The (..)
Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. heart auscultation (aortic stenosis); c. Until then, I consider any of these to be independent adverse riskfactors. -- Finally, a dedicated syncope unit may improve evaluation and outcome (17). Good History and Physical exam, including a.
We evaluated the primary outcome (cardiovascular death, myocardial infarction, or hospitalization for unstable angina, heart failure, or resuscitated cardiac arrest) and other end points, by sex, in 1168 (22.6%) women and 4011 (77.4%) men. of invasive‐assigned men, and no ≥50% stenosis in 12.3% of invasive‐assigned men;P<0.001).
Demographic characteristics, vascular riskfactors, and the results of preoperative serum biochemistry were measured and collected. The riskfactors for vulnerable carotid plaque were analyzed. A Lasso-logistic regression prediction model was developed and compared with traditional logistic regression models.
There is a trend toward these patients being younger with a greater relative percentage of women and fewer traditional cardiac riskfactors. As I wrote in that Nov.
42% of adults are considered obese , increasing their risk of diabetes, hypertension, and cardiovascular issues. Additionally, 10% of the global population suffers from chronic kidney disease , with diabetes and hypertension as significant riskfactors. In the U.S.,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content