This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Hospital evaluation for this patient was negative for an acute coronary syndrome ( ie, CT coronary angiogram was normal — troponin was not elevated — and Echo was negative, with no sign of pericardial effusion ). The patient was discharged with a diagnosis of acute pericarditis — and treated with a full course of colchicine and ibuprofen.
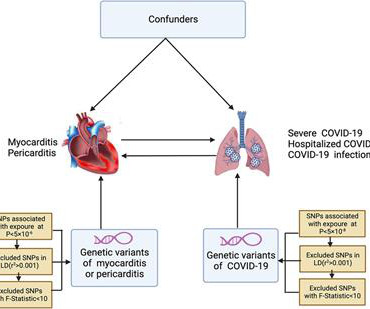
Background & aims Coronavirus disease 2019 (COVID-19) is strongly associated with myocarditis or pericarditis risk in observational studies, however, there are still studies that do not support the above conclusion. Results Non-associations in the IVW and sensitivity analyses were observed for COVID-19 with myocarditis or pericarditis.
Background Coronavirus disease (COVID-19)-associated acute pericarditis has recently received much attention owing to its high frequency associated with pericardial tamponade (PT), showing unfavorable prognosis. Conclusions We encountered a unique case of COVID-19-associated acute pericarditis exhibiting hemorrhagic PT.
"New study shows corticosteroid use may increase pericarditis recurrence in lupus patients. Researchers recommend caution with oral prednisone treatment to lowe
Pericarditis refers to inflammation of the pericardium The pericardium is a sac within which the heart sits. Acute inflammation of this sac is known as acute pericarditis. About 5% of patients who present to A+E with chest pain which is not deemed to be a heart attack or angina are ultimately diagnosed with pericarditis.
She presented to an outside hospital after several days of malaise and feeling unwell. This is a value typical for a large subacute MI, n ormal value 48 hours after myocardial infarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). Electrocardiographic diagnosis of postinfarction regional pericarditis Oliva PB.
This rules out pericarditis, which essentially never has reciprocal ST depression. This is not pericarditis because: a. Pericarditis does not have reciprocal depression. ST elevation of pericarditis is maximal in leads II and V5, V6. Pericarditis does not have hyperacute T-waves.
The case reports Case 1 involves a 26 year old man who developed pericarditis after the Pfizer vaccine. Pericarditis, an inflammation of the sac the heart lives in, developed about 7 days after the Pfizer vaccine. She has had multiple repeat hospital presentations and 2 months later continues to be symptomatic.
They informed me that she had just been hospitalized 10 days ago for "some fluid around the heart" and was discharged after one day without incident. Ultimately, she spent several days in the hospital and no further fluid collected. She was diagnosed with pericarditis and spent one day in the hospital without events.
Pericarditis? If you were thinking that this is pericarditis, that would be possible in the absence of any clinical information. However, there is zero PR depression which would be VERY unusual in pericarditis. P.S.: Acute pericarditis may produce diffuse ST elevation. Presence of STD is helpful; absence is not.
Prolonged chest pain calls for early hospitalization and you have to attend the hospital emergency room. Driving alone to the hospital should be avoided at all costs as it can be catastrophic. Another type of pain originating from the heart is due to an inflammation of its covering known as pericarditis.
These latter findings are typical of pericarditis, but pericarditis never has reciprocal ST depression. Despite active CP — cath lab activation was deferred and this patient was transported to a local hospital without PCI capability. Usually with pericarditis and myocarditis — hyperacute T waves (HATW) are not present.
He was seen at another hospital and found to have a slightly elevated troponin, then underwent a CT pulmonary angiogram (PE) protocol which revealed a right sided pneumonia. Echo does not necessarily differentiate acute MI from pericarditis: both may have wall motion abnormalities. He was treated with Ceftriaxone and azithromycin.
Post-infarction Regional Pericarditis (PIRP) PIRP happens when MI is transmural, all the way from subendocardium to subepicardium, thus leading to inflammation of the subepicardium (next to the pericardium). MYOCARDIAL RUPTURE AND POSTINFARCTION REGIONAL PERICARDITIS KEY POINTS · Myocardial rupture occurs in 1 to 1.5% Re-occlusion 2.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of Chest Pain and Dyspnea Head On Motor Vehicle Collision. Between 81-95% of life-threatening ventricular dysrhythmias and acute cardiac failure occur within 24-48 hours of hospitalization.
Postablation chest pain consistent with pericarditis was reduced with colchicine (4% versus 15%; HR, 0.26 [95% CI, 0.09–0.77];P=0.02) years, colchicine did not reduce a composite of emergency department visit, cardiovascular hospitalization, cardioversion, or repeat ablation (29 versus 25 per 100 patient-years; HR, 1.18 [95% CI, 0.69–1.99];P=0.55).CONCLUSIONS:Colchicine
Given his exertional chest pain and elevated troponin, the patient was admitted to the hospital for "NSTEMI" with a plan for left heart catheterization the next day. Dyspnea, Chest pain, Tachypneic, Ill appearing: Bedside Cardiac Echo gives the Diagnosis 31 Year Old Male with RUQ Pain and a History of Pericarditis.
On day 3 of hospitalization she underwent coronary angiography, revealing a 95% lesion in the mid-LAD which was stented. The second troponin I returned elevated at 6.4, and for some reason there were no more troponins measured after that. One can say with full confidence that is was completely occluded at the time of the presentation ECG.
A previously healthy 53 yo woman was transferred to a receiving hospital in cardiogenic shock. Well, don't we see diffuse ST Elevation in Myo-pericarditis (with STD in aVR)? This was sent by a reader. and K was normal. Here was the ECG: There is sinus tachycardia. This is "Shark Fin" morphology. So this is STEMI, right? Which artery?
Pericarditis is rare — but myocarditis is not , so especially in this age group — more information is needed to quickly determine if this could be an acute MI, myocarditis, or none of the above. The patient arrested outside the hospital. Unfortunately — the cardiologist at that center did not recognize the abnormal ECG findings.
This is a bad ST vector orientation, because it causes widespread STE and one of the most important mistakes that needs to be avoided here is thinking of the diagnosis of pericarditis. Such an out-of-proportion STE is virtually never seen in pericarditis. He arrived to our hospital one hour later.
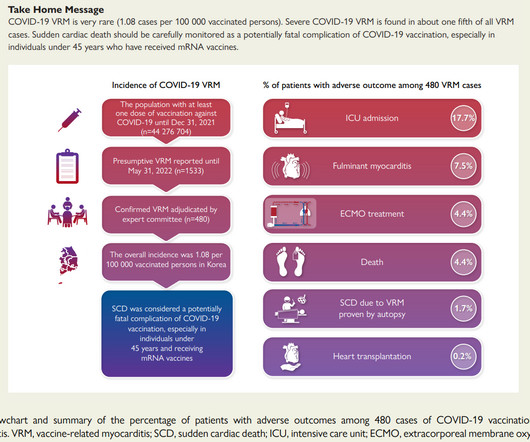
The KDCA also established a reporting system with a legal obligation for special adverse events including myocarditis and pericarditis after COVID-19 vaccination. While there have been case reports published of severe VRM, Israeli and US data found no severe cases in their published series.
She was discharged after a short hospitalization with oncology and cardiology follow-up. The second most common cause of medical cardiac tamponade is acute idiopathic pericarditis. Fluid samples were sent for culture and cytology and results showed malignant cells. A repeat POCUS showed resolution of her pericardial effusion.
He spent almost 2 months in the hospital, and reportedly made a full neurologic recovery. Dyspnea, Chest pain, Tachypneic, Ill appearing: Bedside Cardiac Echo gives the Diagnosis 31 Year Old Male with RUQ Pain and a History of Pericarditis. This patient arrested shortly after hospital arrival. He was prescribed apixaban.
As always, takotsubo cardiomyopathy and focal pericarditis can mimic OMI, but takotsubo almost never mimics posterior MI, and both are diagnoses of exclusion after a negative cath. We have countless cases of missed posterior MI on this blog, including these: Interventionalist at the Receiving Hospital: "No STEMI, no cath.
Another handy section is for troponin levels and their delta cut-offs, which can be modified according to the kit used in your hospital. We would like to thank Muzaffer Değertekin, MD, PhD, Prof. President Elect) and Bülent Mutlu, MD, Prof. Associate General Secretary ) of Turkish Society of Cardiology, for their support.
To Emphasize: When the patient is older and presents with a history of cardiac-sounding chest pain — then acute infarction will be much more common than acute pericarditis, myocarditis, or perimyocarditis. F ollow- U p in T oday's C ASE: The patient in today's case was diagnosed as having acute myocarditis.
You do NOT see this in normal variant STE, nor in pericarditis. After admission to the hospital, the patient was discharged from the hospital without any investigation of his acute MI. Here is the computer interpretation: (Veritas algorithm) This is what I said: "This is diagnostic of an acute inferior MI.
Further Reading: [link] See these relevant cases: A man in his 50s with acute chest pain and diffuse ST depression "Pericarditis" strikes again Is it important to recognize LVH Pseudo-infarction patterns? Wonderfully, she has returned to her normal life with no significant co-morbidities from her dissection.
Amazingly, he did not suffer any serious complication in hospital. This is the most important exception to the classic teaching of "diffuse STE without reciprocal depression is less likely ACS, more likely pericarditis". He recovered and was discharged several days later. Long term follow up is unknown at this point.
He was then transferred to quaternary care childrens hospital. Pericarditis? No apical thrombus noted using Definity contrast. Coxsackie serologies negative. Covid PCR negative. UDS positive for marijuana only. There, troponins were trended up to 100,000 ng/L (still unknown if troponin I or T). Beware a negative Bedside ultrasound.
To-date no larger studies have assessed sub-clinical myocardial mechanics in acute tuberculous pericarditis (ATBP) and age/sex/ethnic differences, and synergistic-prognostic association of these parameters with patients' outcomes (survival).Aim:To
4 An accompanying editorial 5 notes “Data from COVID-Heart provide reassuring evidence that myocarditis, once predicted to be an emerging public health crisis attributable to COVID-19, is relatively uncommon even among hospitalized patients and is less virulent than predicted during the early days of the pandemic.
Written by Kirsten Morrissey, MD with edits by Bracey, Grauer, Meyers, and Smith An older teen was transferred from an outside hospital with elevated serum troponin and and ECG demonstrating ST elevations. The workup at the transferring hospital yielded elevated troponin I at 18.1 Acute coronary syndrome in a pediatric patient?
To perform these interventions, a team of 8 Ngaliema Clinic staff went to Christian Barnard Memorial Hospital, Cape Town where they were trained by Dr Susan Vosloo. Two diasporan members of AFMED have been operating patients at the Monkole Hospital Centre and Kinshasa University Clinic during the summer.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content