This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System. The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB.
He presented with chest pain, not relieved by nitro, pain reproducible on exam and centered around the pacemaker insertion site. is very specific for STEMI , and there is some evidence, as well as rationale, that a paced rhythm behaves similarly. Here is one case of anterior STEMI in a paced rhythm.
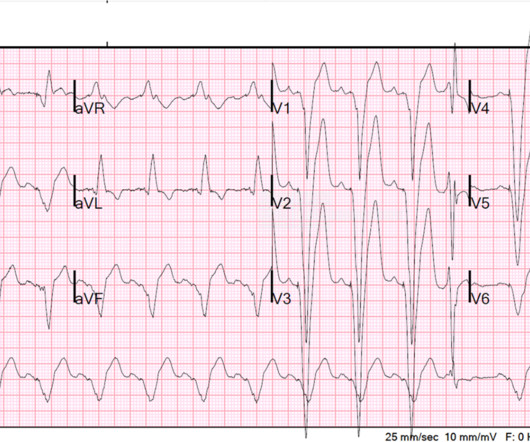
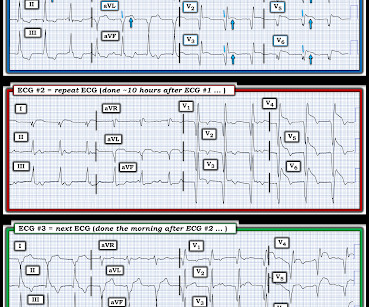
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. The patient was extubated on Day-3 of the hospital stay. The patient improved, and on Day-11 of the hospital stay — he was off inotropes and on a small dose of a ß-blocker. The below ECG was recorded.
There is STE in III and aVF which does not meet STEMI criteria due to insufficient STE in lead aVF. The interventionalists insisted that the ECGs did not meet STEMI criteria and cancelled the activation, stating that they would consider urgent cath after further stabilization. This is an obvious inferoposterior OMI.
The patient was promptly admitted to the hospital for further evaluation. Again, see Ken's discussion below) Discussion continued The absence of pace spikes suggests this is not a pacemaker/ICD-related rhythm in this patient with an ICD. An initial electrocardiogram (ECG) is provided below. What do you think? What is the rhythm?
According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician. A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. It’s important to stress the presence of a normal QRS (i.e.,
There is clearly sufficient STE for STEMI criteria in leads V2 and aVL, but lead I has less than 1.0 mm of STE - thus, technically this ECG does not meet STEMI criteria, although it is a quite obvious OMI. This ECG was immediatel y discussed with the on-call cardiologist who said the ECG was "concerning but not a STEMI."
This case was sent by Dr Avinash Krishnamurthy, a fine emergency medicine resident from Australia Cairns base hospital Case : An adolescent male had a mechanical fall and injured his left shoulder and arm. Is there STEMI? A Patient with Ischemic symptoms and a Biventricular Pacemaker His chest was tender. What is it?
Anterior STEMI? Referral to the patient’s primary care clinician ( added as an essential part of this patient’s hospital discharge instructions ) — can facilitate optimal longterm management ( and hopefully avoid recurrent ED visits in the future for the same problem ). What is it? Activate the Cath Lab?
His initial cTnI at the receiving hospital was 27 ng/mL, and no further troponins were measured thereafter. Unfortunately there is no echocardiogram accessible because the patient checked himself out of the hospital in order to get back to his home state before it could be completed. To our knowledge, the patient did well.
The medics recorded the following initial ECG at time 0: The computer read (see below) gives no further comment beyond ventricular pacemaker. About 10 minutes later, and shortly before arrival at hospital (NOT Hennepin!), BOTTOM LINE: Despite cardiac pacing — ECG #2 is diagnostic of a very large acute anterior STEMI.
Learning Points: Ectopic atrial rhythm can produce atrial repolarization findings that can be confused for acute ischemia, STEMI, or OMI. Because of its potential for invoking uneeded cardiac catheterization or hospital admission — it is worth periodically reviewing this ECG pattern.
Abnormal ST elevation is also seen in the high-lateral limb leads ( = leads I and aVL ) which together with the abnormal ( and very large ) Q waves and QS complexes in 8/12 leads suggests that the reason for this ventricular rhythm is a recent and/or ongoing extensive antero-lateral STEMI. What Then is the Rhythm in Figure-4?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content