This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This narrative review aims to evaluate strategies for reducing door-to-balloon (D2B) time in ST-elevation myocardial infarction (STEMI) patients, focusing on pre-hospital, in-hospital, and technological innovations, as well as addressing challenges to ensure sustainability.
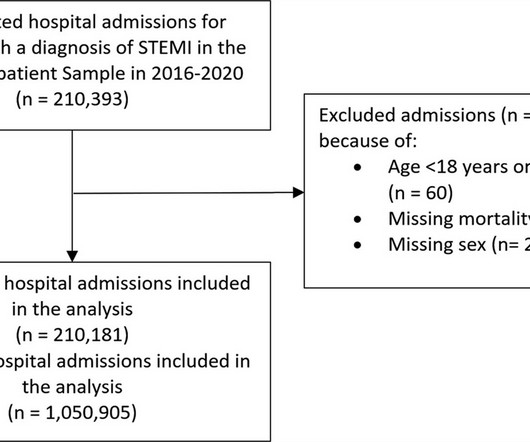
Background It is unclear how COVID-19 pandemic affected care and outcomes among patients who are diagnosed with ST-elevation myocardial infarction (STEMI) in the USA. Results There were 1 050 905 hospitalizations with STEMI, and there was an 8.2% of hospitalizations had a diagnosis of COVID-19, and the mortality was 11.5%
Later it was shown that index of microvascular resistance which quantified the inability of microcirculation to vasodilate and improve coronary flow after primary PCI, was associated with worst outcomes independent of epicardial coronary flow. Immediate Microvascular Physiology After Mechanical Coronary Reperfusion of STEMI.
See these 2 articles Association between pre-hospital chest pain severity and myocardial injury in ST elevation myocardial infarction: A post-hoc analysis of the AVOID study Author links open overlay panel [link] 1 Background We sought to determine if an association exists between prehospital chest pain severity and markers of myocardial injury.
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? This is the response he got: Interventionist: "No STEMI, no cath. After stabilizing the patient and recording more ECGs, he tried again: Interventionalist: "It isn't a STEMI." It is a STEMI equivalent. We don't know how many though.
Written by Jesse McLaren Three patients presented with acute chest pain and ECGs that were labeled by the computer as completely normal, and which was confirmed by the final cardiology interpretation (which is blinded to patient outcome) also as completely normal. What do you think?
BackgroundThe pharmacoinvasive (PhI) strategy is the standard-of-care for ST-elevation myocardial infarction (STEMI) patients when primary percutaneous coronary intervention (pPCI) is unfeasible. Multivariable logistic regression models were used to assess the association between lysis-PCI timing and outcomes.
Jason was very skeptical of STEMI. This also argues against STEMI. What was the outcome? Outcome "I later found out that this is a patient who regularly calls paramedics to c/o chest pains and he had fooled many of them. He complained of 3 days of diarrhea and abdominal pain. What do you think? Jason, I agree.
Frailty and CVD are often interrelated, affecting disease and treatment outcomes. Frailty is a syndrome of physiological decline, characterized by marked vulnerability to adverse health outcomes. Patients were categorized as frail if they had a hospital frailty risk score (HFRS) of 5 or higher, and non-frail if their score was below 5.
Background Despite advances in percutaneous coronary intervention (PCI) for ST segment elevation myocardial infarction (STEMI), in-hospital mortality remains a concern, highlighting the need for the identification of additional risk factors such as serum iron levels. μmol/L) and a control group (Fe ≥7.8 μmol/L).
This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System. The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB.
As a low-volume PCI centre in the Middle East, we wanted to find out if the outcomes of our PCI procedures are different from those of high-volume PCI centres in the UK and the Western world. Prospectively collected data of all comers for PCI (urgent and elective) were retrospectively analysed. and the average number of stents 2.6.
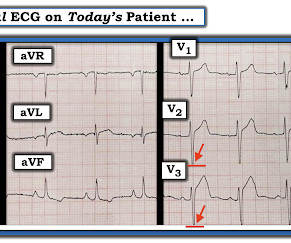
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Circulation 2007 2. Khan et al.
STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al. References: 1. Available from: [link] [link] 2.
Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Day 12 ECG: FINAL DIAGNOSIS: "NSTEMI" Despite the fact that his day 4 ECG easily meets STEMI criteria, the patient is diagnosed as NSTEMI. Long term outcome unknown but obviously bleak.
He was admitted to the hospital for a "rule out." His ECG was repeated at this point: This shows a well developed anterior STEMI. To not see these findings is very common, and this patient would be given the diagnosis of NonSTEMI, with subsequent development of STEMI. His first troponin was normal. Fesmire et al.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). As far as I can tell, there is only one randomized trial of immediate vs. delayed intervention for transient STEMI. Labs ordered but not yet drawn.
Data sources Linked Clinical Practice Research Datalink (CPRD) and Hospital Episode Statistics (HES). Interventions Aspirin and clopidogrel (AC, reference) versus aspirin and prasugrel (AP) or aspirin and ticagrelor (AT); AP evaluated only in patients with ST-elevation myocardial infarction (STEMI). Setting Primary and secondary care.
However, the true benefits are hidden in a timely early reperfusion, best done at out-of-hospital (or even in-hospital*) with the emergency crew’s assistance. In this context, we need a movement to revive the pre-hospital thrombolysis. In LAD STEMI time is more crucial. This is what CAPTIM told us.
He was admitted to the hospital for evaluation of these symptoms — but no ECG was done at that time. At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). The rest of the patient’s hospital stay was uneventful and he was eventually discharged. The proximal LAD is now widely patent.
Inflammatory indicators such as neutrophil count and monocyte count potentially may predict patients’ outcomes and prognosis in ACS. Data was collected from patients and their medical records during hospital stay using a structured data collection form. Rate of MACE as composite outcome 30-days after PPCI as 24.7% (n=37).
His friend was able to get him into the truck and drive him to a nearby community hospital (non-PCI center). Is this inferor STEMI? Atrial Flutter with Inferior STEMI? The EM provider asked if the cardiologist thought it was a "STEMI." Long-term outcome is unknown. Tachycardia and ST Elevation.
Now let’s compare this with the existing paradigm to identify multiple preventable delays to reperfusion, which can be improved through the paradigm shift from STEMI to OMI. In the STEMI paradigm, patients with ischemic symptoms and ECGs that don’t meet STEMI criteria get serial ECGs. There are no measurements that are reliable.
Non-randomized trials show better outcomes (neurologic survival) using this device; see this article in Resuscitation: Head and Thorax Elevation during cardiopulmonary resuscitation using circulatory adjuncts is associated with improved survival. Finally, head-up CPR (which was not used here), makes for better resuscitation.
Jason was very skeptical of STEMI. This also argues against STEMI. What was the outcome? Outcome "I later found out that this is a patient who regularly calls paramedics to c/o chest pains and he had fooled many of them. Look for old ECGs Do serial ECGs Do echocardiography June 17, 2016 Anterior STEMI?
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. Could there have been a different outcome if the crews immediately recognized OMI – versus a shortened PR-interval – and commenced with pre-hospital Cath Lab activation? Is this OMI?
Wuhan Asia Heart Hospital, Wuhan, China Did you guess the diagnosis correctly? We know, how adverse is the outcome of Left main STEMI. Video source and courtesy: Leizhi Ku,, Xiaojing Ma, From the Departments of Radiology (L.K.) and Echocardiography (X.M.), But, the true diagnosis is different. It is left main atresia.
There is clearly sufficient STE for STEMI criteria in leads V2 and aVL, but lead I has less than 1.0 mm of STE - thus, technically this ECG does not meet STEMI criteria, although it is a quite obvious OMI. This ECG was immediatel y discussed with the on-call cardiologist who said the ECG was "concerning but not a STEMI."
Another ECG was recorded 5 minutes later just before arrival at the hospital: Similar The patient was transported to a nearby suburban hospital with PCI capabilities while my partner cared for her. This has resulted in an under-representation of STEMI MINOCA patients in the literature. She was defibrillated and resuscitated.
Jason asked me if I thought it is due to occlusion (without either of us knowing the outcome), and this was my answer: This is a posterolateral MI. Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Therefore it is not a STEMI. Some are STEMI-equivalents.
The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Current Emergency and Hospital Medicine Reports (2013) 1:4352.
These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? Appropriately, the physicians repeated the ECG 20 minutes later and it was diagnostic of anterior STEMI. Outcome : The third troponin I, drawn 4.5
Despite active CP — cath lab activation was deferred and this patient was transported to a local hospital without PCI capability. It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. Patient #1 in today's post did not get expert ECG interpretation.
This case was sent by Dr Avinash Krishnamurthy, a fine emergency medicine resident from Australia Cairns base hospital Case : An adolescent male had a mechanical fall and injured his left shoulder and arm. Is there STEMI? There was apparently no syncope and he had no bony injuries, but he did complain of left sided chest pain.
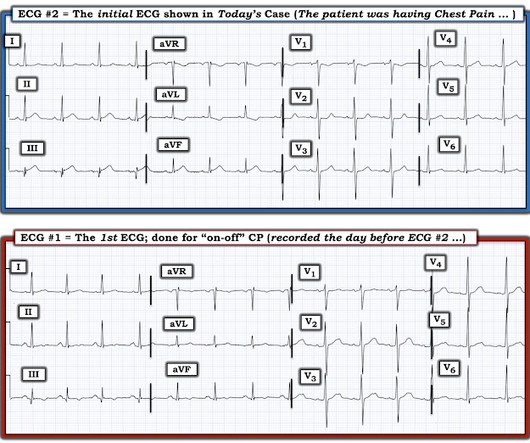
It is difficult to describe exactly why, but is something that simply comes with time, after following up hundreds of cases to see the ECG progression and patient/angiographic outcomes. This one likely does meet STEMI criteria in II, III, and aVF. Criteria for a STEMI are definitely not met in ECG #1. What is the ECG Diagnosis?
Post by Smith, with short article by Angie Lobo ( [link] ), a third year intermal medicine resident at Abbott Northwestern Hospital Case A 30-something woman with no past history, who is very fit and athletic, presented with 1.5 It is equivalent to a transient STEMI. hours of substernal chest pressure. She had zero CAD risk factors.
Here is PM Cardio's Queen of Hearts interpretation (AI ECG interpretation trained by Meyers, Smith, and PM Cardio team using thousands of cases and their outcomes): The output number ranges from 0 to 1, with numbers closer to zero meaning likely NOT OMI, and numbers closer to 1 meaning OMI.
The patient was started on dual antiplatelet therapy and discharged from the hospital on day 3 without further event. Recall that air is a poor conductor of electricity and will, therefore, generate smaller amplitudes on posterior leads (hence why STEMI criteria requires only >0.5 mm in any posterior lead to be considered positive).
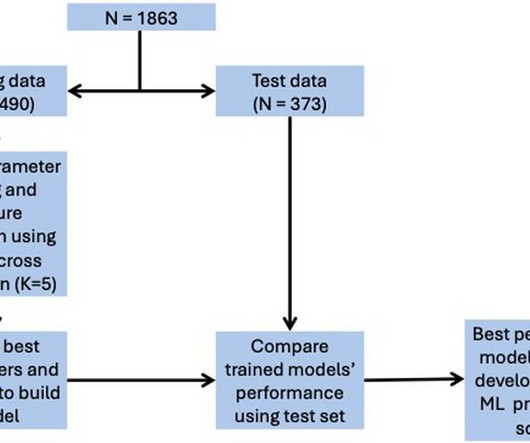
Final models were chosen to optimise area under the curve (AUC) score while ensuring interpretability.ResultsOverall, 128 (6.9%) patients died in hospital, with 292 (15.7%) patients requiring ICU admission and 373 (20.0%) patients with LVEF < 40%. for in-hospital mortality, 0.78 for ICU admission, and 0.74 for LVEF < 40%.
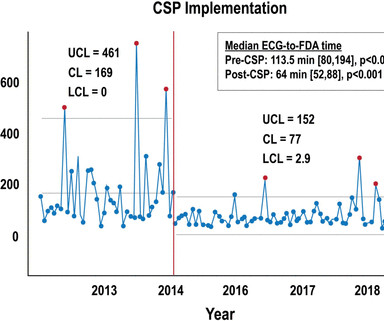
Background Patients who experience in-hospital ST-segment elevation myocardial infarction (iSTEMI) represent a uniquely high-risk cohort owing to delays in diagnosis, prolonged time to reperfusion and increased mortality. Key metrics and clinical outcomes were compared before and after CSP implementation. to 76.5% (p=0.04).
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? The patient stabilized and had a good outcome. to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5 The corrected QT interval is extremely long, about 500 ms. If the patient is at 1.8,
I sent this ECG to the Queen of Hearts (PMcardio OMI), and here is the verdict: You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form Then I learned that a Code STEMI was activated for concern of anterior "STEMI" in V1-V2. High sensitivity troponin I was 23 ng/L.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content