This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
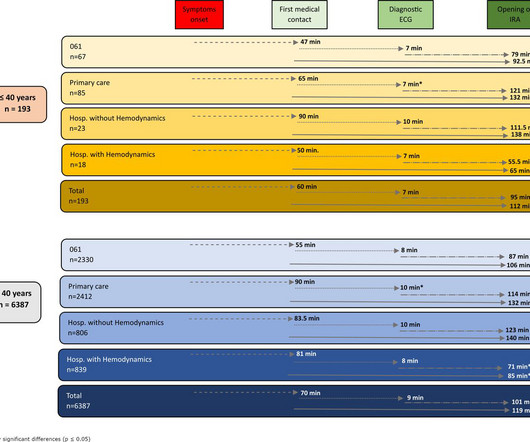
Introduction ST-elevation myocardialinfarction (STEMI) is one of the most prevalent presentations in young patients. Methods A retrospective, multicentre cohort study was carried out in 6799 patients diagnosed with STEMI. to 2.06) (p<0.001) or going to a hospital without haemodynamics (RR 1.55, 95% CI 1.45
This narrative review aims to evaluate strategies for reducing door-to-balloon (D2B) time in ST-elevation myocardialinfarction (STEMI) patients, focusing on pre-hospital, in-hospital, and technological innovations, as well as addressing challenges to ensure sustainability.
However, whether immediate blood glucose and FIB levels affect coronary blood flow during primary percutaneous coronary intervention (PCI) remains unclear.ObjectiveTo explore the correlation between admission blood glucose (ABG), fibrinogen (FIB) and slow blood flow during primary PCI for acute ST segment elevation myocardialinfarction (STEMI).MethodsA
Background The diagnosis of a left ventricular (LV) thrombus in patients with ST-segment elevation myocardialinfarction (STEMI) remains challenging. Methods We retrospectively evaluated 337 consecutive STEMI patients. All patients underwent transthoracic echocardiography (TTE) and CMRI during their index hospitalization.
See these 2 articles Association between pre-hospital chest pain severity and myocardial injury in ST elevation myocardialinfarction: A post-hoc analysis of the AVOID study Author links open overlay panel [link] 1 Background We sought to determine if an association exists between prehospital chest pain severity and markers of myocardial injury.
Background Early recognition of ST-segment elevation myocardialinfarction (STEMI) is needed for timely cardiac monitoring and reperfusion therapy. The national cardiac (ANZACS-QI) registry and national administrative datasets capture all New Zealand public hospital admission diagnoses and mortality data.
IntroductionHypoxic liver injury (HLI) and Killip classification are poor prognostic factors in patients with ST-segment elevation myocardialinfarction (STEMI). In-hospital mortality was directly related to Killip classification (2.3%, 7.3%, 16.3%, 29.2%) with statistical significance.
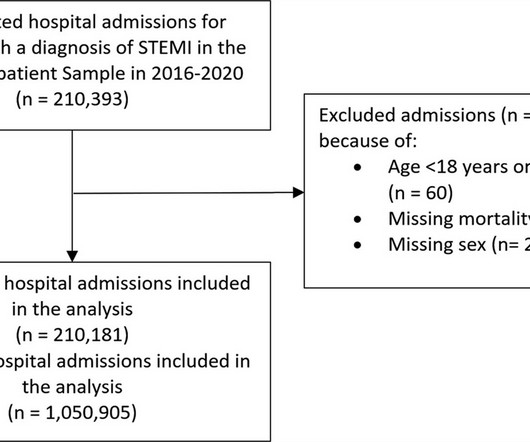
Background It is unclear how COVID-19 pandemic affected care and outcomes among patients who are diagnosed with ST-elevation myocardialinfarction (STEMI) in the USA. Results There were 1 050 905 hospitalizations with STEMI, and there was an 8.2% reduction in admissions in 2020. reduction in admissions in 2020.
BackgroundThere may be variability in willingness to perform percutaneous coronary intervention (PCI) in higherrisk patients who present with STsegmentelevation myocardialinfarction (STEMI). We compared patientlevel characteristics of patients who did and did not undergo PCI at each hospital. versus 7.4%,P<0.001),
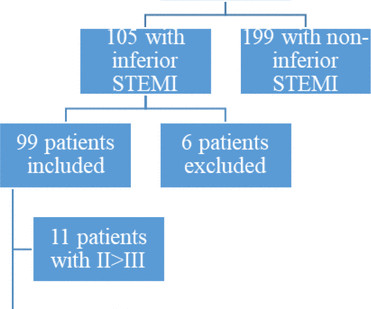
Background ST elevation myocardialinfarction (STEMI) represents a cardiac emergency. Inferior STEMI represents a dilemma for cardiologists. Methods We performed a single-centre retrospective cohort analysis of all patients admitted to our hospital from 2008 to 2020 with a diagnosis of inferior STEMI.
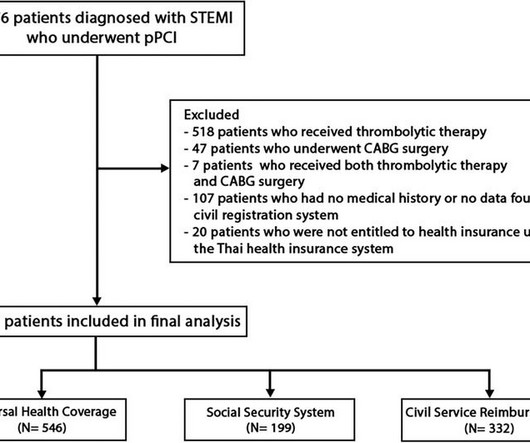
BackgroundIn Thailand, access to specific pharmaceuticals and medical devices for ST-elevation myocardialinfarction (STEMI) patients is restricted within certain healthcare systems, leading to inequalities in the quality of medical care among different healthcare systems.
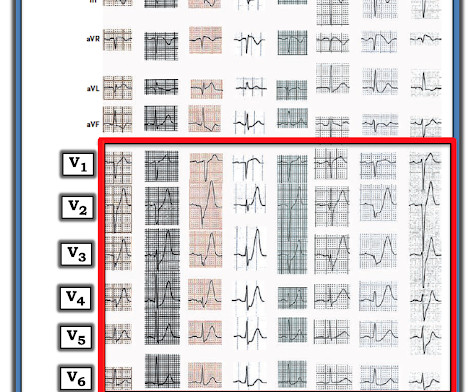
Written by Pendell Meyers I received this prehospital ECG (we receive prehospital ECGs by telemetry from EMS in a large area around our hospital) and was told that there was a patient in her 50s with chest pain who was headed to an outside hospital (which happens to be a catheterization center). Here is the ECG: What do you think?
BackgroundThe pharmacoinvasive (PhI) strategy is the standard-of-care for ST-elevation myocardialinfarction (STEMI) patients when primary percutaneous coronary intervention (pPCI) is unfeasible. Optimal timing for post-fibrinolytic PCI (lysis-PCI) remains elusive.
This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System. The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB.
BackgroundCurrent research suggests that microvascular obstruction (MVO) following the first percutaneous coronary intervention (PCI) in myocardialinfarction patients is closely related to inflammatory responses. The predictive model incorporating LCR enhances the ability to predict MVO occurrence in patients with STEMI post-PCI.
Background Despite advances in percutaneous coronary intervention (PCI) for ST segment elevation myocardialinfarction (STEMI), in-hospital mortality remains a concern, highlighting the need for the identification of additional risk factors such as serum iron levels. μmol/L) and a control group (Fe ≥7.8 μmol/L).
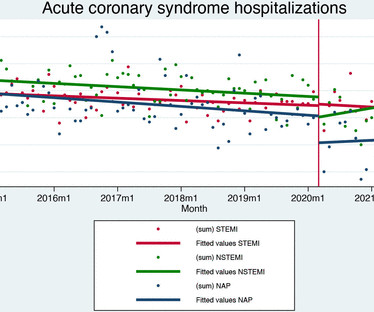
Aims We evaluated the effects of the COVID-19 pandemic on hospital admission and quality of care for acute coronary syndrome. Data on 21 001 patients were included (7057 ST-elevation myocardialinfarction (STEMI), 7649 non-ST elevation myocardialinfarction (NSTEMI) and 6295 unstable angina).
The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI"). I advised that perhaps posterior leads would help to persuade the interventionalist, since the 2022 ACC recommendations include posterior STEMI as a formal STEMI equivalent, but only officially by 0.5
It is now well known that even if a coronary artery is opened well after a myocardialinfarction, with good flow in the epicardial coronary arteries, there could be impaired myocardial perfusion. Immediate Microvascular Physiology After Mechanical Coronary Reperfusion of STEMI. J Am Coll Cardiol. van Leeuwen, Stephen P.
The Society of Cardiovascular Angiography and Interventions has published an expert consensus statement on the management of patients with ST-elevation myocardialinfarction.
She presented to an outside hospital after several days of malaise and feeling unwell. This is a value typical for a large subacute MI, n ormal value 48 hours after myocardialinfarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). At the time of admission, her vital signs were normal. Hammill SC.
Background:Little is known about the clinical relevance of interleukin (IL)-6 and the severity of patients with acute ST-elevation myocardialinfarction (STEMI). Blood samples for biomarker analyses, including IL-6, were collected.Results:There were 64 consecutive STEMI patients. There was 75% of males.
Purpose Construction of a prediction model to predict the risk of major adverse cardiovascular events (MACE) in the long term after percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardialinfarction (STEMI).
He has now implemented the Queen of Hearts in his hospital. The emergency physician asked the advice of Dr. Reiters because of absence of STEMI criteria. Translation from French: Acute Occlusion MyocardialInfarction with High Confidence. This case was sent by Dr. Jean-christophe Reiters, an interventionalist in Belgium.
Is primary PCI superior to thrombolysis in the first hour of STEMI ? Steg PG, Bonnefoy E, Chabaud S, Lapostolle F, Dubien PY, Cristofini P, Leizorovicz A, Touboul P; Comparison of Angioplasty and Prehospital Thrombolysis In acute Myocardialinfarction (CAPTIM) Investigators. No, it is not. Read ref 1, 2. Reference 1.
OMI Pocket Guide The OMI Pocket Guide ( [link] ) is a user-friendly online resource designed to help healthcare professionals learn how to recognize subtle signs of acute coronary occlusion on the ECG which represent occlusion myocardialinfarctions (OMI). I’ve accessed this hand OMI Pocket Guide on both my ipad and iphone.
The cardiologist recognized that there were EKG changes, but did not take the patient for emergent catheterization because the EKG was “not meeting criteria for STEMI”. Diagnosis of Type I vs. Type II MyocardialInfarction in Emergency Department patients with Ischemic Symptoms (abstract 102). Murakami MM. Smith: What???!!!
associated typical MyocardialInfarction therapies such as statins and ACE inhibitors with significantly decreased 1 year mortality in MINOCA patients, which suggests that they do indeed have a similar pathophysiology to MI patients with obstructive coronary disease. MINOCA I do not have the bandwidth here to write a review of MINOCA.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Circulation 2007 2. Khan et al.
Triage ECG (no prior for comparison): Computer algorithm read: "Sinus rhythm, low voltage QRS, inferior myocardialinfarction, probably old." Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). He reported a normal stress test a few years ago.
However, the true benefits are hidden in a timely early reperfusion, best done at out-of-hospital (or even in-hospital*) with the emergency crew’s assistance. In this context, we need a movement to revive the pre-hospital thrombolysis. In LAD STEMI time is more crucial. This is what CAPTIM told us.
Data sources Linked Clinical Practice Research Datalink (CPRD) and Hospital Episode Statistics (HES). Interventions Aspirin and clopidogrel (AC, reference) versus aspirin and prasugrel (AP) or aspirin and ticagrelor (AT); AP evaluated only in patients with ST-elevation myocardialinfarction (STEMI).
He was admitted to the hospital for a "rule out." His ECG was repeated at this point: This shows a well developed anterior STEMI. To not see these findings is very common, and this patient would be given the diagnosis of NonSTEMI, with subsequent development of STEMI. His first troponin was normal. Fesmire et al. Marti D et al.
The question is Link to the article Check whether your answers concur with this crucial query from Harvard Medical School and Massachusetts General Hospital. We need to de-list the vast majority of chronic ischemic,non-ischemic, or systemic causes of Troponin leaks from the myocardialinfarction chart. What can be done for it?
He was treated for infection and DKA and admission to hospital was planned. Aslanger's pattern (Smith was co-author on this): A new electrocardiographic pattern indicating inferior myocardialinfarction The next troponin returned at 8822 ng/L. Here is the ECG at that point in time: The ischemia is mostly resolved.
Post-procedural data included average length of in-hospital stay, intra-hospital morbidity and mortality, and mortality or admission with ACS 12–36 months after the index procedure. A total of 567 patients underwent coronary catheterisation for the three-year period between January 2018 and December 2020.
This was sent by : Jacob Smith, DO Emergency Medicine Resident Ohio Health Doctors Hospital Emergency Residency Christopher Lloyd, DO, FACEP Director of Clinical Education, USACS Midwest Case A 30 year old patient presents to triage with chest pain. This is diagnostic of inferior MI, though does not meet millimeter criteria for "STEMI."
So we activated the Cath Lab Angiogram: Impression and Recommendations: Culprit for the patient's anterior ST segment myocardialinfarction and out of hospital V-fib cardiac arrest is a thrombotic occlusion of the mid LAD The first troponin returned barely elevated at 36 ng/L (URL = 35) In our study of initial troponin in STEMI, 26.8%
As myocardialinfarction (MI) and many other diagnoses (for example left ventricular hypertrophy, prior MI etc.) Furthermore, some ECGs may not meet the STEMI criteria but may still be diagnostic for acute coronary occlusion (ACO). We would like to thank Muzaffer Değertekin, MD, PhD, Prof.
ng/mL (ULN = 0.030 ng/mL) , diagnostic of myocardial injury. The "criteria" for posterior STEMI are 0.5 Acute myocardial injury: Is it myocardialinfarction, or perhaps myocarditis? Is it STEMI or NonSTEMI? The troponin I returned at 4.1 mm STE in one lead. There is zero ST Elevation. This includes: 1.
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardialinfarction, or any prior PCI/stent. It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. No appreciable skin pallor. Is this OMI?
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
Despite active CP — cath lab activation was deferred and this patient was transported to a local hospital without PCI capability. The ECG is diagnostic of occlusion myocardialinfarction (OMI). It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content