This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The ECG in Figure-1 — was obtained from a middle-aged woman with positional tachycardia and diaphoresis with change of position from suprine to sitting. My THOUGHTS on the ECG in Figure-1: The rhythm is sinus tachycardia at ~105/minute ( ie, The R-R interval is regular — and just under 3 large boxes in duration ).
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Are you confident there is no ischemia? Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Is this: 1.
The ECG shows severe ischemia, possibly posterior OMI. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. The patient was brought to the ED and had this ECG recorded: What do you think? And what do you want to do?
His confusion progressively dissipated enroute to the hospital. Many of the changes seen are reminiscent of LVH with “strain,” and downstream Echo may very well corroborate such a suspicion, but since the ECG isn’t the best tool for definitively establishing the presence of LVH, we must favor a subendocardial ischemia pattern, instead.
He was treated for infection and DKA and admission to hospital was planned. This is ischemic ST depression, and could be due to increasing tachycardia, with a heart rate over 130, but that is unlikely given that the patient is now complaining of crushing chest pain and that there was tachycardia all along. Aslanger's pattern.
The 12-lead ECG and long lead II rhythm strip shown in Figure-1 — was obtained from a previously healthy, elderly woman who collapsed in the hospital parking lot. At about this point in the process — I like to take a closer LOOK at the 12-lead tracing, to ensure there is no acute ischemia or infarction that might need immediate attention.
A few days into her hospital stay she developed chest discomfort and the following ECG was recorded. The ECG below was on file and was taken a few days earlier, on the day of admission to the hospital. The above ECGs show the initiation and continuation of a polymorphic ventricular tachycardia. What do you think?
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
She presented to an outside hospital after several days of malaise and feeling unwell. Sinus tachycardia has many potential causes. This is especially true for the elderly patient with sinus tachycardia. What is the cause of the sudden tachycardia? At the time of admission, her vital signs were normal.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Between 81-95% of life-threatening ventricular dysrhythmias and acute cardiac failure occur within 24-48 hours of hospitalization. Sinus Tachycardia ( common in any trauma patient. ).
The patient was promptly admitted to the hospital for further evaluation. While the initial impression might not immediately suggest ventricular tachycardia (VT), a closer examination raises suspicion. An initial electrocardiogram (ECG) is provided below. What do you think? What is the rhythm? The rate is 132 bpm. What is the rhythm?
His friend was able to get him into the truck and drive him to a nearby community hospital (non-PCI center). We have also shown several cases in which atrial flutter hides true, active ischemia. Tachycardia and ST Elevation. Tachycardia to this degree can cause ST segment changes in several ways. Is this inferor STEMI?
DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR. Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58).
He was admitted to the hospital for evaluation of these symptoms — but no ECG was done at that time. The patient’s angiogram should have been expedited, but the EKG change was not recognized as recurrence of transmural ischemia. The conventional computer algorithm called “ sinus tachycardia, otherwise normal EKG ”.
On hospital day 3, the patient had recurrence of symptoms and the following EKG was obtained. This proves effective treatment of the recurrent ischemia. The patient had no further symptoms of ischemia. EKG 3 is diagnostic for developing re-occlusion, and EKG 4 proves that the nitrates relieved the ischemia. =
It should be known that each category can easily manifest the generic subendocardial ischemia pattern. In general, subendocardial ischemia is a consequence of global supply-demand mismatch that usually ameliorates upon addressing, and mitigating, the underlying cause. What’s interesting is that the ECG can only detect ischemia.
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. The differential of a regular narrow QRS tachycardia is sinus tachycardia, SVT, and atrial flutter with regular conduction. Now the patient is in sinus tachycardia. Her initial EKG is below. Adenosine worked.
A previously healthy 53 yo woman was transferred to a receiving hospital in cardiogenic shock. Here was the ECG: There is sinus tachycardia. Our chief of cardiology, Gautam Shroff, interprets it differently and thinks this is indeed ischemia. This was sent by a reader. and K was normal. This is "Shark Fin" morphology.
Whether these EKGs show myocarditis, a normal variant, or something else, they are overall not typical of transmural ischemia of the anterior or high lateral walls. Patient 1 remained in the hospital overnight. He had multiple episodes of bradycardia and nonsustained ventricular tachycardia.
The ECG shows sinus tachycardia, a narrow, low voltage QRS with alternating amplitudes, no peaked T waves, no QT prolongation, and some minimal ST elevation in II, III, and aVF (without significant reciprocal STD or T wave inversion in aVL). It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia.
The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." Here is the patient's troponin I profile: These were interpreted as due to demand ischemia, or type II MI. ng/mL is seldom a result of demand ischemia (type 2 MI). First was 2.9
The ECG was incorrectly interpreted as no signs of ischemia. Admitted to the hospital service for further evaluation and management." Artificial intelligence can be trained to recognize subtle OMI = My Comment by K EN G RAUER, MD ( 2/6 /2023 ): = The initial ECG in today's case was incorrectly interpreted as, "No signs of ischemia".
These findings are concerning for inferior wall ischemia with possible posterior wall involvement. His initial cTnI at the receiving hospital was 27 ng/mL, and no further troponins were measured thereafter. C linically — the rhythm we see in the long lead II of ECG #3 behaves similar to MAT, even though there is no tachycardia.
Central illustration: In those presenting With monomorphic VT, undergoing coronary ischemia assessment was associated With improved 12-month event-free survival from the primary endpoint of VT recurrence, ICD therapy, heart failure hospitalization, and death. vs 51.5%, respectively, p =0.01).
ECG is consistent with severe hypokalemia and/or hypomagnesemia causing prolonged QT (QU) at high risk of Torsades (which is polymorphic ventricular tachycardia in the setting of a long QT interval). The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course.
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
En route to the hospital the patient experienced multiple short-lasting episodes, with cramping and loss of consciousness. There is a run of polymorphic ventricular tachycardia — which given the QT prolongation, qualifies as Torsades de Points ( TdP ). I measure the RR interval at 795ms and the QT interval at 475ms.
The patient was extubated on Day-3 of the hospital stay. The patient improved, and on Day-11 of the hospital stay — he was off inotropes and on a small dose of a ß-blocker. This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ).
MY Interpretation of Today's Initial ECG: I've labeled key findings in Figure-2 for today's initial ECG: The rhythm is sinus tachycardia at ~105/minute. The sinus tachycardia is a definite concern that something acute may be ongoing. The patient arrested outside the hospital. Figure-2: I've labeled t he initial ECG.
Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. There is no evidence of infarction or ischemia. The patient was given furosemide and admitted to the hospital. An ECG was recorded: This shows a regular narrow complex tachycardia at a rate of about 160. So what is it?
There is sinus tachycardia (do not be fooled into thinking this is VT or another wide complex tachycardia!) A repeat ECG was performed: An interesting mix of subendocardial ischemia pattern AND precordial swirl LAD OMI pattern. OMI and subendocardial ischemia patterns can both be present at the same time.
In terms of ischemia, there is both a signal of subendocardial ischemia (STD max in V5-V6 with reciprocal STE in aVR) AND a signal of transmural infarction of the inferior wall with Q wave and STE in lead III with reciprocal STD in I and aVL. He spent almost 2 months in the hospital, and reportedly made a full neurologic recovery.
If there is polymorphic VT with a long QT on the baseline ECG, then generally we call that Torsades, but Non-Torsades Polymorphic VT can result from ischemia alone. See here for management of Polymorphic Ventricular Tachycardia , which includes Torsades. If there is a pulse, you would call it Torsades. However, the mean level (2.50.4
The terminology favored to describe these ECG findings is diffuse subendocardial ischemia ( See ECG Blog #271 — for more on diffuse subendocardial ischemia ). The reason for this is simple — Most such patients die quickly , usually before they reach the hospital. Quite literally — You can see almost anything!
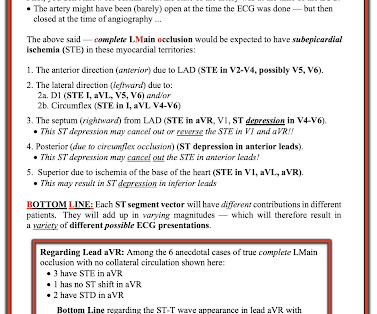
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" That said, complete LM occlusion would be expected to have subepicardial ischemia (STE) in these myocardial territories: STE vector 1.
Patients use them to observe their heart activity by themselves when they are not in the hospital. Though their accuracy is not as high as a hospital ECG machine, they are very beneficial in detecting problems in any medical emergency and providing information about long-term heart activity.
The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. 2] But there is also Sinus Tachycardia! No calcium was administered during pre-hospital transport. Chapter 6: Introduction to Myocardial Ischemia and Infarction. 2] Birnbaum, Y.,
3 studied 416 patients hospitalized with COVID in China, of whom 82 had an initial cTn(I) above the upper reference limit. Association of Cardiac Injury With Mortality in Hospitalized Patients With COVID-19 in Wuhan, China. Prevalence and Impact of Myocardial Injury in Patients Hospitalized with COVID-19 Infection.
Although the shock is no doubt partly a result of poor pump function, with low stroke volume, especially of the RV, it should be compensated for by tachycardia. RCA ischemia often results in sinus bradycardia from vagal reflex or ischemia of the sinus node. This is a perfect indication for atropine. Learning Points : 1.
After initiating treatment for hyperkalemia, repeat ECG showed resolution of Brugada pattern: The ECG shows sinus tachycardia. A Very Wide Complex Tachycardia. These include ( among others ) — acute febrile illness — variations in autonomic tone — hypothermia — ischemia/infarction/cardiac arrest — and Hyperkalemia.
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. Evidence of acute ischemia (may be subtle) vii. Most physicians will automatically be worried about these symptoms. Left BBB vi.
The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. However, there is also significant tachycardia , with heart rate of 116, and known hypoxia. Cardiology services were consulted at a PCI capable hospital. An EKG was immediately recorded.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















































Let's personalize your content