This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This EKG is diagnostic of transmural ischemia of the inferior wall. If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia. Transmural ischemia (as seen with the OMI findings on ECG) is not very common with demand ischemia, but is possible. Smith SW.
The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI"). I advised that perhaps posterior leads would help to persuade the interventionalist, since the 2022 ACC recommendations include posterior STEMI as a formal STEMI equivalent, but only officially by 0.5
About 20 minutes later ( on the way to the hospital ) — the patient's CP resolved, and ECG #1 was recorded. mmm ECG Blog #193 — Reviews the concept of why the term “OMI” ( = O cclusion-based MI ) should replace the more familiar term STEMI — and — reviews the basics on how to predict the " culprit " artery.
The ECG shows severe ischemia, possibly posterior OMI. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. Cardiac arrest #3: ST depression, Is it STEMI? And what do you want to do? Figure-1: The initial ECG in today's case. —
See these 2 articles Association between pre-hospital chest pain severity and myocardial injury in ST elevation myocardial infarction: A post-hoc analysis of the AVOID study Author links open overlay panel [link] 1 Background We sought to determine if an association exists between prehospital chest pain severity and markers of myocardial injury.
This is a 45 yo male who had an inferior STEMI 6 months prior, was found to have severe LAD and left main disease, and was supposed to be set up for CABG a few weeks later, but did not follow up. But it could be anterior STEMI. 40% of anterior STEMI has upward concavity in all of leads V2-V6. is likely anterior STEMI).
Below is the first ECG recorded by paramedics after 2 hours of chest pain, interpreted by the machine as “possible inferior ischemia”. While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. What do you think?
He was treated for infection and DKA and admission to hospital was planned. Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present. They agreed ischemia was likely in the setting of demand given DKA and infection. 40 mg of furosemide was given.
These tall T waves are associated with flattening ( straightening ) of the ST segment in the inferior leads — with slight S T elevation in leads V2-thru-V6 ( albeit not enough to qualify as a "STEMI" — Akbar et al, StatPearls, 2023 ). About 20 minutes later ( on the way to the hospital ) — the patient's CP resolved, and ECG #1 was recorded.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR.
This suggests further severe ischemia. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al.
Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. and repeat the ECG, to see if the apparent ischemia persists. A third ECG was done about 25 minutes after the first: This shows resolution of all apparent ischemia.
His friend was able to get him into the truck and drive him to a nearby community hospital (non-PCI center). We have also shown several cases in which atrial flutter hides true, active ischemia. Is this inferor STEMI? Atrial Flutter with Inferior STEMI? The EM provider asked if the cardiologist thought it was a "STEMI."
She presented to an outside hospital after several days of malaise and feeling unwell. It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI. At the time of admission, her vital signs were normal. Heart rate was in the 80s.
Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Smith : the profound persistent STE suggests either persistent occlusion or " no reflow " with persistent downstream ischemia. Long term outcome unknown but obviously bleak.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. His response: “subendocardial ischemia. Anything more on history? POCUS will be helpful.”
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. Whether these EKGs show myocarditis, a normal variant, or something else, they are overall not typical of transmural ischemia of the anterior or high lateral walls.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. Alternatively, it is a variant of diffuse subendocardial ischemia, with STE in V1 reciprocal to ST depression in inferior and lateral leads.
My interpretation was: RBBB with hyperacute T-waves in V4-V6 that are all but diagnostic of LAD occlusion vs. post ROSC ischemia. The patient had ROSC and maintained it. A 12-lead ECG was obtained: What do you think?
These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). While this may be change that is reciprocal to an Acute/Subacute Inferior STEMI, the problem is that LV aneurysm may also manifest with this reciprocal change. In STEMI, they are generally upright and large in proportion to the QRS. This case is tough.
He was admitted to the hospital for evaluation of these symptoms — but no ECG was done at that time. At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). The patient’s angiogram should have been expedited, but the EKG change was not recognized as recurrence of transmural ischemia.
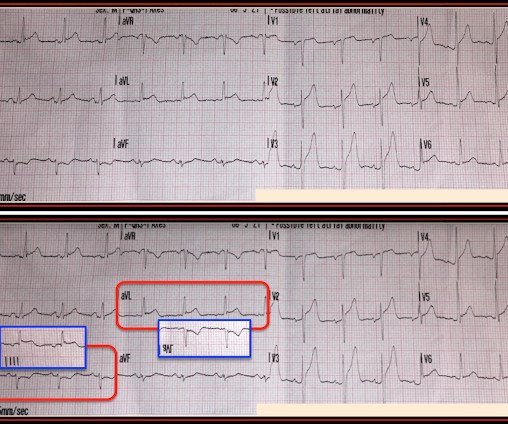
Down-up T-waves in inferior leads are almost always reciprocal to ischemia in the territory underlying aVL. This is not normal and is a tip off that there is posterior ischemia accompanying the ischemia in aVL. Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet.
Prehospital ECG: Obvious anterolateral STEMI (Proximal LAD occlusion) The cath lab was activated prehospital by the medics. Perhaps they indicate an open artery with minimal flow and severe subendocardial ischemia, but not total subepicardial ischemia. Interventionalist at the Receiving Hospital: "No STEMI, no cath.
The patient was promptly admitted to the hospital for further evaluation. Learning Point: Concordant ST segment elevation can arise from profound ischemia triggered by ventricular tachycardia (VT), or it may represent an exaggerated basal ST change accompanying tachycardia. An initial electrocardiogram (ECG) is provided below.
A previously healthy 53 yo woman was transferred to a receiving hospital in cardiogenic shock. So Shark Fin really is just a dramatic representation of STEMI, and can be in any coronary distribution. So this is STEMI, right? Our chief of cardiology, Gautam Shroff, interprets it differently and thinks this is indeed ischemia.
The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Similarly, STEMI guidelines call for urgent angiography for refractory ischemia or electrical/hemodynamic instability, regardless of ECG findings. Refractory ischemia or electrical/hemodynamic instability are indications for the PCI.
There is broad subendocardial ischemia as demonstrated by STE aVR with concomitant STD that almost appears appropriately maximal in Leads II and V5. There is LBBB-like morphology with persistent patterns of subendocardial ischemia. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital.
This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI. Figure-2: TOP — Initial ECG obtained pre-hospital.
Here it is: The computer reads STEMI What do you think? More from the medic: "LifePak 15 interpretation was STEMI. Transmitted to hospital with PCI." "ER My response: "I think it is very worrisome for STEMI." It meets STEMI criteria even for a male under age 40, with STE 2.84 Pattern looked to be BER.
This meets "STEMI criteria" However, there is very high voltage, with a very deep S-wave in V2 and tall R-wave in V4. The morphology is not right for STEMI. My interpretation: LVH with secondary ST-T abnormalities, exaggerated by stress, not a STEMI. This is very good evidence that the ST elevation is not due to STEMI.
The HEART and EDACS scores are helpful to risk stratify patients with chest pain, but they hinge on accurate ECG interpretation: a low score doesn’t apply if the ECG shows STEMI(+)OMI, and shouldn’t be used for STEMI(-)OMI or OMI reperfusion either 2. Was this objective evidence of inducible ischemia accompanied by chest pain?
KEY Point: In areas of the heart where an acute STEMI produces ST elevation — reperfusion T waves ( that develop after the "culprit" artery reopens ) will appear as T wave inversion. The C ASE C ontinues : En route to the hospital — another tracing was done 2 minutes after ECG #1. ECG Blog #367 — for another example of acute LCx OMI.
Post by Smith, with short article by Angie Lobo ( [link] ), a third year intermal medicine resident at Abbott Northwestern Hospital Case A 30-something woman with no past history, who is very fit and athletic, presented with 1.5 It is equivalent to a transient STEMI. It they are static, then they are not due to ischemia.
According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician. A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. It’s important to stress the presence of a normal QRS (i.e.,
There is STE that does not meet STEMI criteria in V1-V6. This patient's ischemia was so brief that it did not cause any myocardial stunning. I focus my attention on the first 2 ECGs, both of which were done prior to arrival in the hospital. This was mistaken by the treating physicians for ST depression initially.
Another ECG was recorded 5 minutes later just before arrival at the hospital: Similar The patient was transported to a nearby suburban hospital with PCI capabilities while my partner cared for her. These findings are diagnostic of an apical OMI as a result of LAD Occlusion. She was defibrillated and resuscitated. From Gue at al.
These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? Appropriately, the physicians repeated the ECG 20 minutes later and it was diagnostic of anterior STEMI. QTc is the computer measurement. 100% LAD occlusion.
I am going to code this as an acute STEMI as he had transient ST elevation which started to evolve in the emergency department but I think this is most appropriately termed STEMI." Is this Acute Ischemia? When is it anterior STEMI? Next day ECG: 2 Very instructive posts on LVH and OMI and Pseudo-OMI 1. More on LVH.
The morphology of STE is not diagnostic of being due to acute transmural ischemia. This one likely does meet STEMI criteria in II, III, and aVF. The development of an inferior-posterior STEMI, from prehospital to hospital Inferior hyperacute T-waves. Criteria for a STEMI are definitely not met in ECG #1.
The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." Here is the patient's troponin I profile: These were interpreted as due to demand ischemia, or type II MI. ng/mL is seldom a result of demand ischemia (type 2 MI). First was 2.9
These findings are concerning for inferior wall ischemia with possible posterior wall involvement. His initial cTnI at the receiving hospital was 27 ng/mL, and no further troponins were measured thereafter. The morphology in V2 is also concerning and it appears that the ST segment is being pushed down, as in ST depression.
Learning Points: Ectopic atrial rhythm can produce atrial repolarization findings that can be confused for acute ischemia, STEMI, or OMI. Because of its potential for invoking uneeded cardiac catheterization or hospital admission — it is worth periodically reviewing this ECG pattern.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















































Let's personalize your content