This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
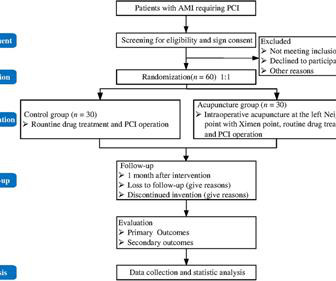
BackgroundSlow flow/no-reflow (SF-NR) during percutaneous coronary intervention (PCI) is associated with poor prognosis of patients with acute myocardialinfarction (AMI). Currently, effective treatment is not available for SF-NR. However, its effects on SF-NR in the AMI patients during PCI are not clear.
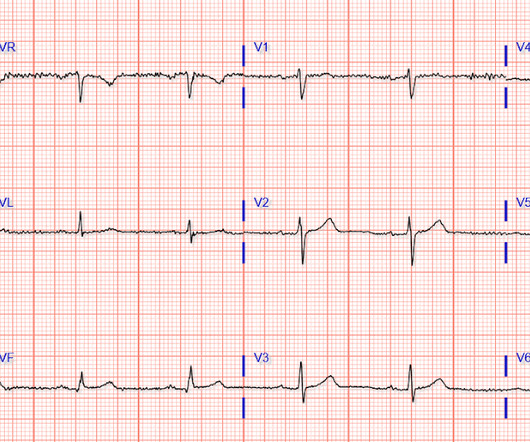
This EKG is diagnostic of transmural ischemia of the inferior wall. Smith: note also the terminal QRS distortion in lead III (absence of S-wave without a prominent J-wave). . __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand).
See these 2 articles Association between pre-hospital chest pain severity and myocardial injury in ST elevation myocardialinfarction: A post-hoc analysis of the AVOID study Author links open overlay panel [link] 1 Background We sought to determine if an association exists between prehospital chest pain severity and markers of myocardial injury.
He was treated for infection and DKA and admission to hospital was planned. Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present. They agreed ischemia was likely in the setting of demand given DKA and infection. 40 mg of furosemide was given.
The patient survived the hospitalization. V5-V6) of any amplitude, is specific for Occlusion MyocardialInfarction (vs. non-occlusive ischemia) Ongoing ischemic symptoms in NSTEMI is already an indication for emergent cath, regardless of the ECG. Peak troponin was not recorded. Long term follow up is unavailable.
Martha Gulati, MD, director of preventive cardiology in the department of cardiology at Los Angeles-based Cedars-Sinai's Smidt Heart Institute has raised awareness of two heart conditions needing better diagnostic tools ischemia with no obstructive coronary arteries and myocardialinfarction with no obstructive coronary arteries.
She presented to an outside hospital after several days of malaise and feeling unwell. This is a value typical for a large subacute MI, n ormal value 48 hours after myocardialinfarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). At the time of admission, her vital signs were normal. Hammill SC.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. The ECG is diagnostic of occlusion myocardialinfarction (OMI).
DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR. Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58).
Background:Myocardial infarction with nonobstructive coronary artery disease (MINOCA) is a special syndrome with clear evidence of myocardialischemia, but no clear stenosis of coronary artery imaging sign. Circulation, Volume 150, Issue Suppl_1 , Page A4143007-A4143007, November 12, 2024.
This suggests further severe ischemia. associated typical MyocardialInfarction therapies such as statins and ACE inhibitors with significantly decreased 1 year mortality in MINOCA patients, which suggests that they do indeed have a similar pathophysiology to MI patients with obstructive coronary disease. Downstream vasospasm?
Triage ECG (no prior for comparison): Computer algorithm read: "Sinus rhythm, low voltage QRS, inferior myocardialinfarction, probably old." Smith : the profound persistent STE suggests either persistent occlusion or " no reflow " with persistent downstream ischemia. He reported a normal stress test a few years ago.
My interpretation was: RBBB with hyperacute T-waves in V4-V6 that are all but diagnostic of LAD occlusion vs. post ROSC ischemia. The patient had ROSC and maintained it. A 12-lead ECG was obtained: What do you think? Smith's ECG Blog — Interpretation of a post-resuscitation ECG can be extremely challenging.
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
of patients had evidence of ischemia on a prior functional test. 1.10];P=0.198), nonfatal myocardialinfarction (RR, 1.09 [95% CI, 0.63–1.88];P=0.768), 1.88];P=0.768), and cardiovascular hospitalizations (RR, 0.91 [95% CI, 0.59–1.39];P=0.669) were referred to CCTA and 22.5% In the follow-up ranging from 1 to 3.5
They had had twice the rate of cardiac arrest and twice the in-hospital mortality[1] In another study of patients diagnosed with STEMI, those on dialysis experienced delayed reperfusion and double the mortality.[2] Clinical characteristics of dialysis patients with acute myocardialinfarction in the United States. Khan et al.
Although radiation into the left arm is most classic for coronary ischemia, radiation into both arms is actually modestly more predictive ). The primary care physician's note indicates low suspicion for cardiac ischemia, but "for completion, check troponin and ECG." If an ECG was obtained in the office, it was not saved.
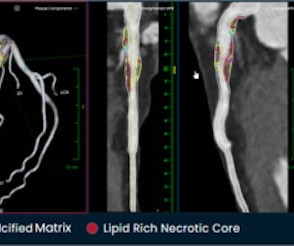
Hafiane, Vulnerable plaque, characteristics, detection, and potential therapies , J. Cardiovasc. 6 (3) (2019). If you enjoy this content, please share it with a colleague
ST-elevation myocardialinfarction after pharmacologic persantine stress test in a patient with Wellens’ syndrome. Single High-Sensitivity Cardiac Troponin I to Rule Out Acute MyocardialInfarction. Evaluating Rapid Rule-out of Acute MyocardialInfarction Using a High-Sensitivity Cardiac Troponin I Assay at Presentation.
Post by Smith, with short article by Angie Lobo ( [link] ), a third year intermal medicine resident at Abbott Northwestern Hospital Case A 30-something woman with no past history, who is very fit and athletic, presented with 1.5 It was late evening and the patient will be in the hospital overnight with a potentially very unstable LAD lesion.
There is broad subendocardial ischemia as demonstrated by STE aVR with concomitant STD that almost appears appropriately maximal in Leads II and V5. There is LBBB-like morphology with persistent patterns of subendocardial ischemia. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital.
Figure-1: Initial ECG, obtained pre-hospital from this 40-ish year old woman with new-onset chest pain ( See text ). Figure-2: TOP — Initial ECG obtained pre-hospital. In view of the lack of J waves in the pre-hospital tracing — it would certainly seen that these J waves were ischemia-induced , and markers of the “culprit artery”.
Another ECG was recorded 5 minutes later just before arrival at the hospital: Similar The patient was transported to a nearby suburban hospital with PCI capabilities while my partner cared for her. Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed Coronary Arteries). Learning Points: 1.
This confirms that there were dynamic signs of ischemia on the initial ECG. ng/ml , a three-fold increase from troponin #2, also confirming acute myocardialinfarction. This patient should be admitted to the hospital — and, at the least — should be cathed at some time during her hospital stay before she goes home.
According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician. Upon hospital arrival, the patient verbalized slight attenuation of pain. It’s important to stress the presence of a normal QRS (i.e., No serial ECG’s were recorded.
The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." Here is the patient's troponin I profile: These were interpreted as due to demand ischemia, or type II MI. ng/mL is seldom a result of demand ischemia (type 2 MI). First was 2.9
He requested transport to the hospital out of an abundance of caution, and all subsequent serial ECG’s showed no changes from Figure 1-2, shown above. The respective hospital course was unremarkable. Terminal QRS distortion is present in anterior myocardialinfarction but absent in early repolarization. Figure 1-2.
In the ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trial, researchers examined the risk of ischemic events in patients with stable coronary artery disease. years, with 57.1% occurring within 30 days after CABG. Original article: Redfors B et al.
Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion MyocardialInfarction (Versus Nonocclusive Ischemia). The patient was started on dual antiplatelet therapy and discharged from the hospital on day 3 without further event. J Am Heart Assoc. 2021 Dec 7;10(23):e022866.
Electrocardiographic Differentiation of Early Repolarization FromSubtle Anterior ST-Segment Elevation MyocardialInfarction. Case 4 Transient STEMI, serial ECGs prehospital to hospital, all troponins negative (less than 0.04 This makes it almost certain that the ST elevation on the first one is due to ischemia.
BackgroundStrain assessed by cardiac magnetic resonance (CMR) is a key prognostic indicator in myocardialinfarction. However, the strain characteristics and prognostic value in myocardialinfarction with nonobstructive coronary arteries (MINOCA) with different causes are unclear.
The impact of this narrowing can ultimately result in angina (chest pain), which has been shown to double the risk of major cardiovascular events,1 as well as myocardialinfarction ( heart attack ) or even death.
If there is polymorphic VT with a long QT on the baseline ECG, then generally we call that Torsades, but Non-Torsades Polymorphic VT can result from ischemia alone. I have read articles that say that patients without ischemia are at low risk of complications from hypokalemia, But it is not entirely without risk. 1987;147(3):465-469.
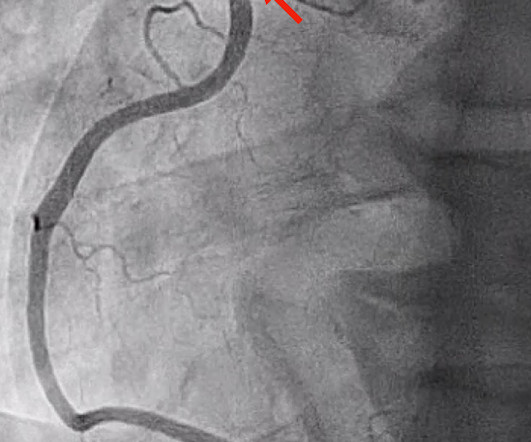
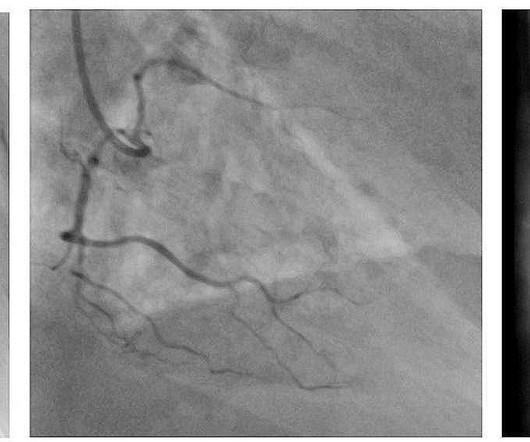
A 53-year-old male presenting emergently with signs of myocardialinfarction received immediate coronary angiography and thoracic CT-scan showing occlusion of the first marginal coronary branch without possibility of revascularization and minimal pericardial extravasation.
A cardiovascular reactivity risk score was calculated by allotting 0 to 3 points for each quartile of increasing abnormality for each of the 3 reactivity responses and summing the quartile points from the MIPS (Mental Stress Ischemia Prognosis Study) to yield a cardiovascular reactivity risk score ranging from 0 to 9.
When “spot diagnosing” precordial ST-depression I instinctively evaluate aVR for any corresponding ST-elevation to see if an emerging pattern of broad subendocardial ischemia can be appreciated, in which the ST-depression should be otherwise global and demonstrably maximal in Leads II and V5. He left AMA and is lost to follow-up. is present.
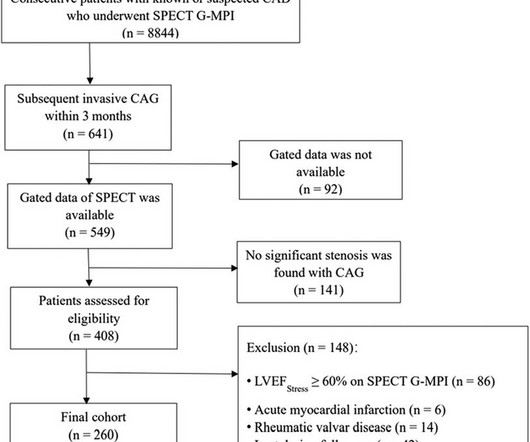
The primary endpoints were major adverse cardiac events (MACEs), a composite of all-cause death, nonfatal myocardialinfarction, unplanned coronary revascularization, and hospitalization for unstable angina.ResultsWe observed 69 MACEs (26.5%).
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" That said, complete LM occlusion would be expected to have subepicardial ischemia (STE) in these myocardial territories: STE vector 1.
V1 sits over both the RV and the septum, so transmural ischemia of either one with give OMI pattern in V1 and reciprocal STD in V5 and V6. The family filed a lawsuit against the physician and the hospital. The hospital and doctor reached confidential settlements. The family elected to switch to comfort care and she died.
The primary endpoint of this study was major adverse cardiovascular and cerebrovascular events (MACCEs) that included all-cause mortality, non-fatal myocardialinfarction, non-fatal ischemic stroke, and ischemia-driven revascularization.Results:The average age of the study participants was 59.55 ± 10.98
Troponin T peaked at 38,398 ng/L ( = a very large myocardialinfarction, but not massive-- thanks to the pre-PCI spontaneous reperfusion, and rapid internvention!! ). The patient was extubated on Day-3 of the hospital stay. There is no definite evidence of acute ischemia. (ie, Inotropic medication was continued.
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. In normal times, the most common use of cTni is in diagnosing, or ruling out, acute myocardialinfarction (AMI, a subcategory of acute myocardial injury.
Study end points include mortality, cardiovascular events (hospitalization for acute myocardialinfarction or stroke) and limb events (hospitalization for critical limb ischemia or major amputation) and were identified using Veterans Affairs and nonVeterans Affairs encounters.ResultsThe mean age was 70.6
The outcome measure was peri-procedural complications defined as a composite of perioperative death, major bleeding, contrast nephropathy, myocardialinfarction, ischemic stroke, and major amputation. Procedure time was categorized into four clinically relevant groups (≤59, 60–119, 120–179, and ≥180 minutes). of the participants.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content