This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
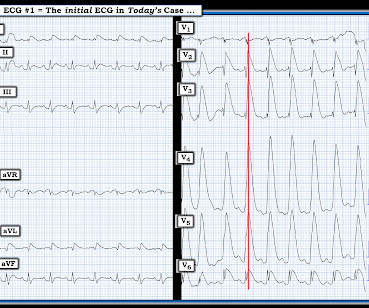
That said — the ECG in Figure-1 should prompt the following considerations: The symmetric chest lead T wave inversion in ECG #1 could be a sign of coronary disease, potentially with acute ischemia. During my decades of working with residents when hospital Attending — by far, the most commonly overlooked vital sign was respiratory rate.
In the ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trial, researchers examined the risk of ischemic events in patients with stable coronary artery disease. years, with 57.1% occurring within 30 days after CABG. Original article: Redfors B et al.
BACKGROUND:Lower-limb amputation rates in patients with chronic limb-threatening ischemia vary across the United States, with marked disparities in amputation rates by gender, race, and income status. 0.98];P=0.019), and those who received care at a safety-net hospital (odds ratio, 0.87 [95% CI, 0.78–0.97];P=0.012) Mean age, 76.6
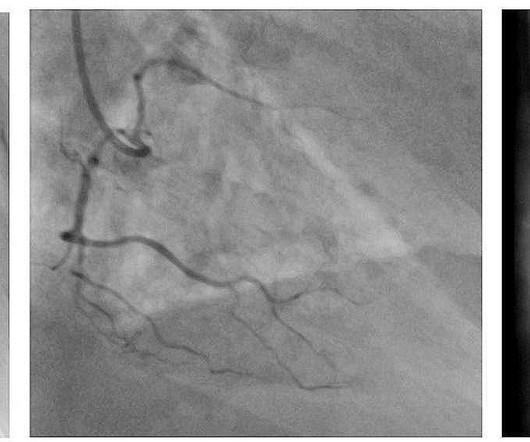
At the hospital, left main coronary-artery stenosis was seen on angiography (shown in a video). In a 57-year-old man with chest pain, an ECG obtained by EMS showed widespread ST-segment depressions.
The ECG shows severe ischemia, possibly posterior OMI. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. The patient was brought to the ED and had this ECG recorded: What do you think? And what do you want to do?
This EKG is diagnostic of transmural ischemia of the inferior wall. If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia. Transmural ischemia (as seen with the OMI findings on ECG) is not very common with demand ischemia, but is possible. Smith SW.
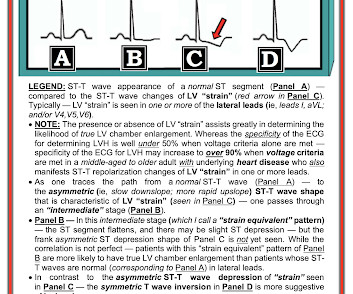
His confusion progressively dissipated enroute to the hospital. Many of the changes seen are reminiscent of LVH with “strain,” and downstream Echo may very well corroborate such a suspicion, but since the ECG isn’t the best tool for definitively establishing the presence of LVH, we must favor a subendocardial ischemia pattern, instead.
In the validation dataset (2,229 patients), the rate of in-hospital mortality was 18.4%. The rate of composite outcome (in-hospital death, stroke/global ischemia, dialysis, and/or acute heart failure) was 41.2%, and 10-year mortality rate was 47.0%.
BackgroundLittle is known about treatment variability across US hospitals for patients with chronic limb‐threatening ischemia (CLTI).Methods All patients aged ≥18 years, admitted to nonfederal US hospitals with a primary diagnosis of CLTI, were identified. Journal of the American Heart Association, Ahead of Print.
ii to show blood flow through the heart muscle and evaluate the presence, extent and degree of myocardial ischemia or infarction. Around 6 million MPI procedures are undertaken each year in theU.S. Flyrcado is now available in selectU.S.markets.
Central illustration: In those presenting With monomorphic VT, undergoing coronary ischemia assessment was associated With improved 12-month event-free survival from the primary endpoint of VT recurrence, ICD therapy, heart failure hospitalization, and death. vs 51.5%, respectively, p =0.01).
He was treated for infection and DKA and admission to hospital was planned. Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present. They agreed ischemia was likely in the setting of demand given DKA and infection. 40 mg of furosemide was given.
About 20 minutes later ( on the way to the hospital ) — the patient's CP resolved, and ECG #1 was recorded. ECG Blog #184 — illustrates the "magical" mirror-image opposite relationship with acute ischemia between lead III and lead aVL ( featured in Audio Pearl #2 in this blog post ). ECG Blog #337 — an OMI misdiagnosed as an NSTEMI.
A prior ECG was available for comparison: Normal One might be tempted to interpret the ST depression as ischemia, but as Smith says, "when the QT is impossibly long, think of hypokalemia and a U-wave rather than T-wave." The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course.
Brittany Weber, MD, PhD , of Brigham and Women’s Hospital, is the 2024 YIA winner for her abstract, "The Frequency, Prevalence, And Outcomes Of Incidentally Detected Coronary Artery Calcium Using Artificial Intelligence Analysis Among Patients With Immune Mediated Inflammatory Diseases.”
Instead, he left the hospital — only to be found dead at home 36 hours later. For full discussion of this case — See ECG Blog #292 — == The 2 ECGs shown in Figure-1 were obtained from a man in his 30s — who presented to the ED ( E mergency D epartment ) with chest pain that began several hours earlier. ECG #2 was recorded 1 hour after ECG #1.
DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR. Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58).
10, 2025 A generous gift of $5 million from Lorraine and Bill Dodero will establish the Lorraine and Bill Dodero Limb Preservation Center at University Hospitals Harrington Heart & Vascular Institute in Cleveland, Ohio. Lorraine and Bill Dodero tim.hodson Fri, 02/14/2025 - 15:33 Feb. When we save a limb, we save a life.
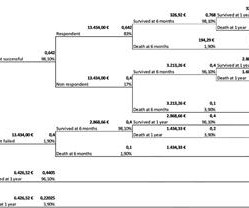
Discussion Whereas the younger patient, who was clinically stable at hospital admission received delayed surgery and did not survive treatment, the older patient, clinically unstable at presentation, went into immediate surgery and had a flawless postoperative course. One year after the operation, he is living at home, symptom free.
He is a Professor of Radiology and prior to joining Cleerly full-time, served as Vice-Chairman of Radiology at George Washington University (GWU) Hospital in Washington, DC. High Diagnostic Accuracy Of AI-Ischemia in Comparison To PET, FFR-CT, SPECT, and Invasive FFR: A PACIFIC Sub-Study. In Press European Heart Journal CV Imag 2024.This
The patient survived the hospitalization. non-occlusive ischemia) Ongoing ischemic symptoms in NSTEMI is already an indication for emergent cath, regardless of the ECG. A woman in her 50s with chest pain and lightheadedness and "anterior subendocardial ischemia" A man in his 50s with acute chest pain who is lucky to still be alive.
The study was aimed to test the effects of GSNO in ischemia/reperfusion (I/R) Injury through relieving thrombo-inflammation.Methods:Male C57BL/6 mice (n=160) were 10-week-old (20-25 g) at the time of surgery. All animals received humane care in compliance with Beijing Tiantan Hospitals guidance.
My written interpretation on a tracing such as this one would read, "Marked LVH and 'strain' and/or ischemia — with need for clinical correlation." BOTTOM LINE: ECG changes of LV "strain" and/or ischemia that we see on today's initial ECG — were not present 9 years earlier. Please see ECG Blog #73 for additional details ).
PCI is commonly used to open blocked arteries to treat significant myocardial ischemia , which occurs when the heart muscle does not get enough oxygenated blood.
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
The "good news" — is that after an extended hospitalization, the patient was finally discharged home, and doing well. = Shark Fin" ST segment elevation is most often a sign of severe transmural ischemia that results from acute coronary occlusion. The ECG in Figure-1 — was obtained following successful resuscitation.
As a result, the ST elevation ( with especially tall, peaked T wave in lead V2) — is not indication of acute ischemia. As suggested by Figure-4 below in the ADDENDUM — assessment of the ST-T waves in leads V2,V3 and V5,V6 — is consistent with ischemia and / or LV "strain". A picture is worth 1,000 words.
FAHA , co-director of the Vascular Center at the University Hospitals Harrington Heart & Vascular Institute and a professor of medicine at Case Western Reserve University School of Medicine , both in Cleveland, Ohio. It has been estimated that less than 5% of patients with PAD in the U.S.
When I was shown this ECG, I said it looks like such widespread ischemia that is might be a left main occlusion, or LM ischemia plus circumflex occlusion (high lateral and posterior OMI). In fact, most do not make it to the hospital alive, which explains why only a tiny percent of OMI are due to full LM occlusion.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Do you agree with this strategy? How can you better assess the ST segments?
Persistent over-dilation of muscle microvasculature may be one cause of chronic limb-threatening ischemia, recent studies by Kuopio University Hospital and the University of Eastern Finland show.
The accuracy to identify ischemia compared with hemorrhage was 0.91 (0.870.93). The main analysis was the accuracy with which they distinguished vascular from nonvascular causes using the discharge diagnosis as a reference.
See these 2 articles Association between pre-hospital chest pain severity and myocardial injury in ST elevation myocardial infarction: A post-hoc analysis of the AVOID study Author links open overlay panel [link] 1 Background We sought to determine if an association exists between prehospital chest pain severity and markers of myocardial injury.
However, many hospitals don't offer thrombectomy because it requires specialist doctors, leaving the majority of patients ineligible for conventional treatment. Histological analysis at 72 hours post-stroke confirmed a significant reduction of edema and area of necrosis in both early and delayed therapy groups.
The patient was extubated on Day-3 of the hospital stay. The patient improved, and on Day-11 of the hospital stay — he was off inotropes and on a small dose of a ß-blocker. There is no definite evidence of acute ischemia. (ie, Some residual ischemia in the infarct border might still be present.
Background Refractory angina (RA) is a chronic condition characterized by the presence of debilitating angina symptoms due to established reversible ischemia in the presence of obstructive coronary artery disease (CAD).
Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. and repeat the ECG, to see if the apparent ischemia persists. A third ECG was done about 25 minutes after the first: This shows resolution of all apparent ischemia.
On hospital day 3, the patient had recurrence of symptoms and the following EKG was obtained. This proves effective treatment of the recurrent ischemia. The patient had no further symptoms of ischemia. EKG 3 is diagnostic for developing re-occlusion, and EKG 4 proves that the nitrates relieved the ischemia. =
A few days into her hospital stay she developed chest discomfort and the following ECG was recorded. The ECG below was on file and was taken a few days earlier, on the day of admission to the hospital. Most such rhythms in the setting of ischemia are VF and will not convert without defibrillation. Acute ischemia?
10, 2025 A generous gift of $5 million from Lorraine and Bill Dodero will establish the Lorraine and Bill Dodero Limb Preservation Center at University Hospitals Harrington Heart & Vascular Institute in Cleveland, Ohio. Lorraine and Bill Dodero tim.hodson Fri, 02/14/2025 - 15:33 Feb. When we save a limb, we save a life.
Dr. Mouaz Al-Mallah, MD, MSc, MASNC, Director of Cardiac PET at Houston Methodist Hospital, said, Flyrcado opens new frontiers for cardiac PET with a significantly longer half-life than existing PET MPI tracers, and we are proud to be one of the first to use it in our cardiac PET lab. National Center for Health Statistics. link] Miller, R.
When flow is restored, wall motion may completely recover so that echocardiogram does not detect the previous ischemia. Even when the serial troponins are negative, the ECG is critical to the diagnosis of ACS. This is not pericarditis because: a. Pain was typical for MI (substernal, not postional or sharp, resolved with NTG) b.
He was intubated in the field and sedated upon arrival at the hospital. This was interpreted by the treating clinicians as not showing any evidence of ischemia. At his family's request, he was transferred to a hospital closer to his home to continue care. They shocked him twice before return of spontaneous circulation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content