This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
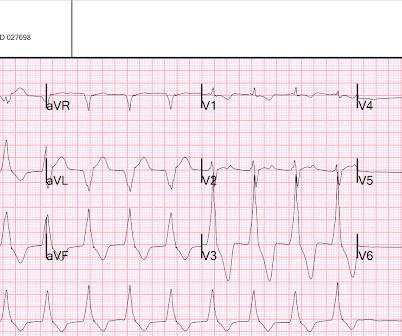
A young man presented with a gunshot wound to the right chest, with hemo-pneumothorax and hemorrhagic shock. There were times when it would be usurped by sinus tachycardia, then return to this rhythm. He got a chest tube and intubation and massive transfusion and stabilized. But he did get an EKG: What is this?
ECG Changes in Intracranial Hemorrhage ECG changes are fairly common in intracranial hemorrhage. Giant T inversions with QT interval prolongation may be seen in intracranial hemorrhage even without associated myocardial damage [1]. But the number of persons with lobar hemorrhage in that study was only 17%. Am Heart J.
Alternatively, it could be posterior fascicular ventricular tachycardia. Either the PSVT was broken and restarted, or there is sinus tachycardia. Maybe the patient has dehydration, sepsis, hemorrhage, or PE. Outcome: The etiology of the patient's sinus tachycardia was not discovered. These are simple and fast.
He was rushed by residents into our critical care room with a diagnosis of STEMI, and they handed me this ECG: There is sinus tachycardia with ST elevation in II, III, and aVF, as well as V4-V6. ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock. He had this ECG recorded. Are the lungs clear?
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
This is the ECG of a 50 yo old woman who collapsed, was found to have a pulse, but then found to be in ventricular tachycardia. Before initiating therapeutic hypothermia, a head CT was done and showed fatal subarachnoid hemorrhage. She was shocked into sinus rhythm. She presented to the ED comatose. This 81 yo was found comatose.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Massive Transfusion for Motorcycle Collision with Hemorrhage, Troponin Elevated. Sinus Tachycardia ( common in any trauma patient. ). He was intubated for altered mental status. Chest trauma was suspected on initial exam.
Side note: The differential of sudden persistent loss of consciousness with adequate hemodynamics is relatively short: seizure, intracranial hemorrhage, basilar artery occlusion. Tachycardia and ST Elevation. There was again no intracranial hemorrhage. Tachycardia to this degree can cause ST segment changes in several ways.
Here is his 12-lead: There is a wide complex tachycardia with a rate of 257, with RBBB and LPFB (right axis deviation) morphology. Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered. See Learning point 1 below. Arch Intern Med.
Interpretation: There is sinus tachycardia, with right bundle branch block (RBBB). 5) Myocardial contusion (edema and hemorrhage in the myocardium) which may result in dysrhythmias, blocks (especially RBBB as here), and poor cardiac contractility, including wall motion abnormalities. She was intubated.
The ECG shows sinus tachycardia, a narrow, low voltage QRS with alternating amplitudes, no peaked T waves, no QT prolongation, and some minimal ST elevation in II, III, and aVF (without significant reciprocal STD or T wave inversion in aVL). It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia.
Systematic Assessment of the ECG in Figure-1: My Descriptive Analysis of ECG findings in Figure-1 is as follows: Sinus tachycardia at ~110/minute. A slightly prolonged QTc ( although this is difficult to assess given the tachycardia ). Initial blood work showed the following: metabolic acidosis on VBG with a lactate of 7.1;
A man in his 40s with multitrauma from motor vehicle collision Massive Transfusion for Motorcycle Collision with Hemorrhage, Troponin Elevated. Sinus Tachycardia ( common in any trauma patient. ). Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ).
Automatic activity refers to enhanced pacemaking function (typically from a non sinus node source), for example atrial tachycardia. below) Other examples of AIVR: Young man with Gunshot wound to right chest with hemorrhagic shock, but bullet path not near heart. The most common triggered arrhythmia is Torsades de Pointes. Bigger et al.
Here is another proven left main occlusion in a young woman who presented with sudden pulmonary edema, had this ECG recorded, then arrested and was resuscitated after 30 minutes of CPR: This has sinus tachycardia with RBBB and LAFB, and STE in V2-V6 as well as I, aVL This pattern could just as easily be seen in LAD occlusion. Knotts et al.
This proves AV dissociation, and by extension ventricular tachycardia. The note lists a diagnosis of "tachycardia," which is described as "narrow complex." (The Repeat ECG obtained in ER: Fortunately for the patient, his ventricular tachycardia spontaneously resolved. Documentation lists a diagnosis of "sinus tachycardia."
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. Also consider non-hemorrhagic volume depletion, dehydration : orthostatic vitals may uncover this [see Mendu et al. (3)].
There was never ventricular fibrillation (VF) or ventricular tachycardia (VT), no shockable rhythm. Moreover, if you know that catastrophic intracranial hemorrhage can result in an ECG that mimics STEMI, then you know that this patient probably has a severe intracranial hemorrhage. There is sinus tachycardia at ~115/minute.
J waves can also be induced by Occlusion MI (5), STEMI mimics including takotsubo and myocarditis complicated by ventricular arrhythmias (6, 7), and subarachnoid hemorrhage with VF (8). The relationship between J wave and ventricular tachycardia during Takotsubo cardiomyopathy.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content