This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
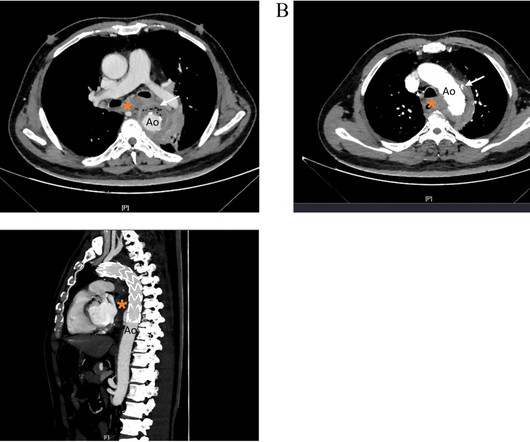
Imaging revealed the presence of an aortic abscess around the stent graft involving the esophagus and mediastinum. The patient's condition deteriorated rapidly after admission, and he ultimately succumbed to hemorrhagic shock. He came to our hospital 6 months later and presented with gastrointestinal bleeding.
BACKGROUND:Carotid artery stenting (CAS) is an alternative treatment for patients with carotid artery stenosis who are not eligible for carotid endarterectomy. The primary outcome was a composite of ischemic stroke, gastrointestinal bleeding, and intracranial hemorrhage within 12 months of switching to single antiplatelet therapy.
Rescue treatment with stenting, balloon angioplasty, and/or intraarterial thrombolysis or antiplatelets are often required to treat the underlying stenosis. 4 Recent literature has reported clinical benefits associated with rescue stenting in the setting of ICAD‐related MT‐refractory strokes.5
In cases of stent-retriever thrombectomy failure, rescue stent angioplasty might be the sole option for achieving permanent recanalization. We defined two binary outcomes: (1) functional clinical outcome (modified Rankin Scale 0-2) and (2) early symptomatic intracerebral hemorrhage (sICH). 10.43, p=0.0325).Conclusions:The
IntroductionVertebral artery stenting represents a viable option in treating symptomatic vertebral artery atherosclerotic stenosis. We included articles reporting patients > 18 years old with symptomatic extracranial vertebral artery stenoses due to atherosclerosis treated with stenting (with or without angioplasty).
3) Rescue stenting (RS) in these patients has shown promising rates of recanalization and better outcomes in preliminary studies. Therefore, rescue stenting can be considered as a safe and viable option in these patients. 1, 2)These patients are also more likely to experience poor functional outcomes. (3)
Background:Studies have demonstrated that the addition of alteplase for patients with tandem lesions who underwent mechanical thrombectomy and acute stenting was safe with improved outcomes. Primary outcomes included symptomatic intracranial hemorrhage (sICH) and parenchymal hematoma type 2 (PH-2). of IV TNK vs 58.2% 105.7], p=0.16).
Herein, we describe a single‐step approach to deploy Neuroform Atlas stent (Stryker Neurovascular, Fremont, CA) which is a hybrid laser‐cut, nitinol self‐expanding stent without the need for ELW or lesion re‐access using MINI TREK RX (Abbott Vascular, Inc., There was no restriction on time from last known well (TLKW) to MT.
BackgroundFor acute proximal intracranial artery occlusions, contact aspiration may be more effective than stent‐retriever for first‐line reperfusion therapy. stent‐retriever versus 55.5% stent‐retriever versus 55.5% stent‐retriever versus 55.5% versus 23.8%;P=0.10). versus 23.8%;P=0.10). versus 23.8%;P=0.10).
Background:Hyperperfusion phenomenon (HPP) constitutes a significant risk factor for adverse outcomes following carotid artery stenting (CAS). Stroke, Volume 56, Issue Suppl_1 , Page ATP178-ATP178, February 1, 2025. Currently, the sole method for evaluating the risk of HPP post-CAS is the invasive acetazolamide (ACZ) challenge test.
Rescue strategies options, including balloon angioplasty alone, rescue stenting (RS) alone, or stent with balloon angioplasty, have shown promise in observational studies and meta‐analyses [3, 4]. The primary efficacy outcome was the shift in the degree of disability, as measured by the modified Rankin Scale (mRS), at 90 days.
Overall, symptomatic intracranial hemorrhage was present in 5.6% (18/326) and mortality in 10.9% (35/326) without difference between first‐line technique.CONCLUSIONIn patients with isolated PCA occlusion, SR was associated with a higher rate of FPE compared with CA or combined techniques with no difference in final successful reperfusion.
Intracerebral hemorrhage (ICH) is a main complication of IVT, with prevalence reported around 3.2% Additionally, extravasation of contrast was seen within the left basal ganglia region, concerning for hemorrhagic transformation from IV‐tPA. He underwent single pass complete recanalization, TICI 2C using Stent retriever and aspiration.
Endovascular intervention was defined as either angioplasty, stenting, or a combination of both. Safety outcomes were comparable with similar rates of symptomatic intracranial hemorrhage (sICH).ConclusionWhile Symptomatic intracranial hemorrhage was low in medically treated patients. Further studies are warranted.
BackgroundProcedural intravenous cangrelor has been proposed as an effective platelet inhibition strategy for stenting in acute ischemic stroke. Safety outcomes included rates of symptomatic intracranial hemorrhage, parenchymal hematoma type 2, petechial hemorrhage, and in‐stent thrombosis. 3.28];P=0.836).
Since then, transfemoral/transradial carotid stenting and transcarotid artery revascularization have emerged as alternatives to endarterectomy for revascularization. Features like intraplaque hemorrhage on MRI and echolucency on B-mode ultrasonography can identify patients at higher risk of stroke with asymptomatic stenosis.
We also compared the safety of acute carotid stenting (CAS) in TLs with low ASPECTS.Methods:This prospective multicenter study from 16 centers included patients with anterior circulation TL from 2015-2020. 5.02; p=0.86), petechial hemorrhages (OR: 0.79, CI: 0.10-6.05; in patients with stenting (18/44) versus no-stenting (25/44).Conclusion:This
We therefore aim to characterize the antiplatelet regimens, and associated thromboembolic/hemorrhagic outcomes, utilized in patients with aneurysms treated with PED Shield.MethodsFactors including demographics, comorbidities, rupture status, devices placed, and antiplatelet regimen, among others, were collected.
Outcomes evaluated include modified Rankin scale at 3 months, symptomatic intracranial hemorrhage, mass effect, 90‐day mortality, and whether any stenting or angioplasty was required during mechanical thrombectomy.Results495 patients met the inclusion criteria out of which 69 had HbA1c of 9% or greater. or greater.
Treatment of ICAS‐LVO with rescue stenting and/or angioplasty has shown promising outcomes, but diagnosing ICAS‐LVO during MT can be challenging [2, 3]. Most respondents (86%) preferred acute treatment of ICAS‐LVO with rescue stenting (RS) +/‐ angioplasty.
Final infarct segmentation included hemorrhagic transformation. ml/h, P = 0.04), a higher likelihood of parent artery stenosis (65% vs. 20.8%, P < 0.001), and increased need for angioplasty or stenting (50% vs. 17%, P < 0.001). The DWI/ADC volume ratio was calculated by dividing DWI volume by ADC 620 10-6 mm2/s volume.
IntroductionThe Advanced Neurovascular Access (ANA5, Anaconda Biomed) is a novel stroke thrombectomy catheter comprising a distal self‐expanding covered funnel designed to locally restrict blood flow in the Internal Carotid Artery (ICA) and, when used in conjuction with available stent retreiver, reduce clot fragmentation during clot ingestion.
carotid stenting) or systemic anticoagulation, hemorrhagic complications, and whom received at least one antiplatelet agent upon discharge. We sought to investigate time-trends and determinants of DAPT prescription after moderate-to-severe NCIS in the Florida Stroke Registry (FSR).Methods:Within
BACKGROUNDThe optimal endovascular approach for acutely ruptured wide‐neck intracranial aneurysms remains uncertain, and the use of stent‐assisted coiling or flow diversion is controversial due to antiplatelet therapy requirements and potential risks. P= 0.180) and hemorrhagic events (WEB: 3.8% Of the patients, 60.5% versus BAC: 2.8%;P=
Time from puncture to recanalization was 68 and 42 minutes, and symptomatic intracranial hemorrhage was significantly different between 1.4% Balloon angioplasty was the treatment technique in 35% and 1.1%, and intracranial stents in 6.4% and 4.2%, while good outcome was similar between 40% and 38%. and 0.05%, respectively.
However, IVT's efficacy on stent retriever (SR) and aspiration thrombectomy (ASP) outcomes specifically remain unclear. Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. IntroductionEfficacy and safety of intravenous thrombolysis (IVT) in patients undergoing mechanical thrombectomy (MT) is still debatable.
IntroductionThe optimal endovascular approach for wide‐neck intracranial aneurysms (IAs) during the acute phase of bleeding remains uncertain, and the use of stent‐assisted coiling or flow diversion is controversial due to antiplatelet therapy requirements and potential risks (1, 2).
Ruptured aneurysmal subarachnoid hemorrhage accounted for 15.7% (8/51) of all patients. There were no hemorrhagic complications. An analysis of the data shows that larger aneurysm dimensions, necessity for adjunctive stent, and minor compaction were significantly associated with inadequate occlusion.
Most respondents (86%) preferred acute treatment of ICAS‐LVO with rescue stenting (RS)±angioplasty. Fear of hemorrhagic complications (74%) was the most compelling reason not to perform RS±angioplasty.
IntroductionObjective: To evaluate the safety and efficacy of the Tigertriever 13 stent retriever in acute ischemic stroke (AIS) patients with primary distal and medium vessel occlusions (DMVO). Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023.
We compared baseline characteristics and completed a one‐way ANOVA to analyze for outcome measures such as in‐hospital mortality, 90‐day mortality, favorable functional outcome defined as modified Rankin Score (mRS) of 0‐2, at 90 days, symptomatic intracranial hemorrhage (sICH) and asymptomatic hemorrhage (aICH) between groups.
Cases of unruptured intracranial aneurysms (UIA) are estimated to affect roughly 3% of the general population and aneurysmal subarachnoid hemorrhage (aSAH) have an incidence of 8 to 9 people per 100,000. IntroductionIntracranial aneurysms, both ruptured and unruptured, pose a significant risk to the general population.
EVT consists of mechanical thrombectomy, thromboaspiration, balloon dilation, stenting, intra-arterial thrombolysis, or various combinations of these methods. Three hundred and forty eligible patients from planned 115 stroke centers in China with AIS of BAO within 4.5
Novel NiTi-braided stent retriever (Venous-TD) is a dedicated venous sinus thrombectomy device. Safety outcomes included peri-procedural complications, all-cause mortality, and symptomatic intracranial hemorrhage after EVT.RESULTS:A total of 61 patients were enrolled and randomized.
Primary effectiveness was complete occlusion (Raymond Roy Class 1) without retreatment at 1-year follow-up (core lab adjudicated), and primary safety was major stroke (ischemic/hemorrhagic) in the territory supplied by the target artery or death.Results:129 cases were included (median age 58 years, IQR: 50-67 years, 85% females). mm (IQR: 4.0-7.5)
Evolucumab group had a higher stent recovery rate than the non‐user group (70.7 However, there were no significant difference in TICI grade, or symptomatic hemorrhage. There were no significant differences between the two groups in age, gender ratio, major risk factors, stroke etiology, or prior statin treatment. vs 53.4%, p = 0.04).
In light of postoperative CT head showing SAH in the basilar, perimesencephalic, prepontine cisterns, interhemispheric fissure and right frontal sulci as well as intraventricular hemorrhage in fourth ventricle, her presentation was thought to be secondary to cerebral vasospasm in the setting of postoperative SAH.
Options include initial angioplasty and/or stenting of the cervical lesion followed by intracranial thrombectomy versus Dotter navigation of catheters through the cervical lesion to first target the intracranial LVO. TICI 2B or greater reperfusion (self‐adjudicated) as achieved in 100% of patients, with a mean time to best TICI of 21 minutes.
Patient underwent emergent mechanical thrombectomy with ADAPT to TICI3 revascularization with future plan for possible angioplasty and stenting of R vertebral stenosis. Initially maintained on aspirin and Cangrelor infusion, then transitioned to aspirin and Plavix without hemorrhagic conversion.
IntroductionPrevious studies did not show a difference in terms of safety and efficacy among first‐line stent retriever (SR), contact aspiration (CA), or combined techniques for proximal large vessel occlusion strokes. Safety measures included procedural complications, symptomatic intracranial hemorrhage (sICH), and 90‐day mortality.
IntroductionThe use of detachable coils for endovascular embolization of cerebral aneurysms has become a safe and effective alternative to direct surgical clipping in patients with ruptured aneurysmal subarachnoid hemorrhage. The post‐procedural complication rate proved to be higher than in non‐ruptured stent‐assisted coiling.
Background:Increased immediate and delayed re-occlusion rates, up to 33%, are reported in patients undergoing acute stenting for tandem lesions, with symptomatic hemorrhage rates around 10-15%. The symptomatic hemorrhage rate was 10.76%, consistent with prior literature. Larger studies are needed to validate these findings.
BACKGROUNDFor patients with acute ischemic stroke (AIS) due to cervical artery dissection (CAD), endovascular stenting can improve and maintain vessel patency for severely stenotic or occlusive lesions. After propensity score matching, 2215 patients remained in the no stenting group, and 2244 remained in the stenting group.
IntroductionCurrent literature suggests a benefit in functional outcomes and reperfusion rates when carotid artery stenting (CAS) and mechanical thrombectomy (MT) are performed emergently. However, rates of symptomatic intracranial hemorrhages have been inconclusive. Stent placement was feasible in all cases.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content