This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Asymptomatic high-grade carotid stenosis is an important therapeutic target for stroke prevention. Features like intraplaque hemorrhage on MRI and echolucency on B-mode ultrasonography can identify patients at higher risk of stroke with asymptomatic stenosis.
Background:Pediatric brain arteriovenous malformation (bAVM) patients often present with intracranial hemorrhage. While certain angioarchitectural features, such as aneurysms, deep venous drainage, a single draining vein, venous outflow stenosis, or small nidus size, increase hemorrhage risk, they do not fully predict it.
Introduction:Literature demonstrates that nearly one-third of acute ischemic stroke (AIS) patients with large vessel occlusion (LVO) or severe stenosis arrive at the emergency room with mild symptoms, attributed to favourable collateral status. Patients who underwent endovascular treatment before END were excluded. 1.22,22.18] P=0.026).Conclusions:Higher
Intracerebral hemorrhage (ICH) is a main complication of IVT, with prevalence reported around 3.2% CT angiography (CTA) showed near occlusive stenosis of the left carotid bulb with an acute thrombus within Supraclinoid Internal Carotid Artery (ICA) extending into the Left MCA and origin of Left Anterior Cerebral Artery (ACA).
Known complications associated with cryoablation include tamponade, phrenic nerve injury, stroke, pulmonary embolism, pulmonary vein stenosis, and atrioesophageal fistulas. Cryoablation for atrial fibrillation is a widely used technique for pulmonary vein isolation.
Iatrogenic complications of endovascular treatment for central venous stenosis have not yet been reported. Here we present a case of a patient on maintenance hemodialysis who developed catheter-related superio.
BACKGROUND:Carotid artery stenting (CAS) is an alternative treatment for patients with carotid artery stenosis who are not eligible for carotid endarterectomy. The primary outcome was a composite of ischemic stroke, gastrointestinal bleeding, and intracranial hemorrhage within 12 months of switching to single antiplatelet therapy.
In cervicocephalic plaques, the ASCVD group had more severe stenosis grades ( p = 0.030) and demonstrated significant differences in LPV, LPR, and CPV ( p = 0.044, 0.030, 0.020) compared with the non-event group. The plaques were then categorized into culprit plaques, non-culprit plaques, and non-event plaques.
The log-rank test demonstrated that patients with the mutation had a higher risk of progression to MMD (P =0.007), stenosis progression (P =0.010), and symptomatic cerebral infarction or hemorrhage (P =0.026). 95% CI, 2.13731;P= 0.001).
Introduction:Moyamoya disease (MMD) is a rare cerebrovascular disease causing nonatherosclerotic intracranial arterial stenosis in children and young adults. This non-terminal ICA stenosis was more frequently observed in Caucasian than in Asian patients (17.5% Stroke, Volume 56, Issue Suppl_1 , Page ATMP11-ATMP11, February 1, 2025.
Background:Assessing carotid artery plaques in stenosis is crucial for treatment strategies and safety. Symptomatic patients or patients with worsening stenosis rates were significantly higher in Group A (75%) than Group B (36%) (p < 0.01).Conclusion:Elevated E-04) compared to non-type VI group (0.70 ± 0.59
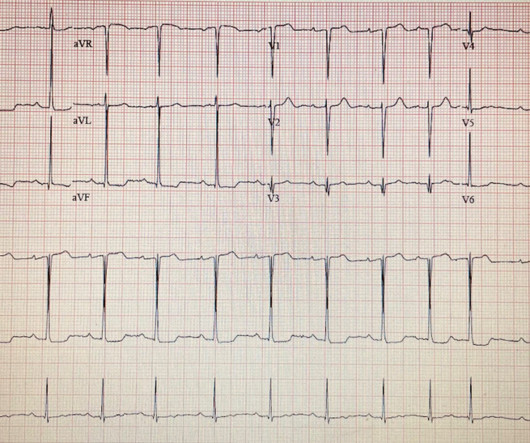
MRI Brain demonstrated Left MCA acute/subacute infarct, MCA/PCA watershed, and no hemorrhagic transformation. No previous medical history was reported. My colleauges and I (interventional cardiology) were asked to consult during workup. Here is the admission ECG.
IntroductionVertebral artery stenting represents a viable option in treating symptomatic vertebral artery atherosclerotic stenosis. The most frequent stenosis location was the V1 segment of the vertebral artery (88.4%). Periprocedural ischemic and hemorrhagic complications occurred in 2.1% The mean age was 65 years, and 74.4%
The patients were categorized into two groups: those with extracranial ICA stenosis and those with occlusion. Clinical outcomes, including functional independence, hemorrhagic events, and procedural time metrics including puncture to reperfusion time were assessed. vs. 50.6%, aOR 1.07, 95% CI 0.70‐1.64, vs. 48.9%, aOR 0.79, 95% CI 0.52‐1.20,
Compared with contralateral carotid artery plaque, plaque burden at the ipsilateral carotid artery was much heavy, presented with a higher degree of stenosis, smaller lumen area (0.22±0.15 Both lumen stenosis and plaque components were correlated with multiple or recurrent infarcts in this population. of them were male.
MRA head demonstrated multifocal arterial stenosis. Repeat CTA head/neck and CT perfusion showed severe stenosis of bilateral M1 segments and left greater than right A1 segments as well as ischemic penumbra in left ACA/MCA watershed territory. Cerebral vasospasm following EEA has rarely been described.
Most neurointerventionalists (91%) diagnose ICAS‐LVO after a continued or recurrent occlusion or by the presence of fixed focal stenosis after multiple mechanical thrombectomy attempts. However, in patients who achieved recanalization with a severe fixed focal stenosis, most (58%) recommended primary medical management.
Methods:This multicenter, observational study recruited first-ever acute ischemic stroke patients attributed to ICAS (>50% stenosis or occlusion) within 7 days after onset. 8.32%), degree of stenosis (60.25±18.95% Patients with recurrent ipsilateral stroke exhibited higher rates of intraplaque hemorrhage (IPH) (30.0%
In our systemic review and meta‐analysis, we included Sixteen dual arm and seven single arm studies in order to study recanalization rate and compare outcomes following rescue stenting in patients with incomplete reperfusion compared to those managed conservatively (no‐RS).(4,
Final infarct segmentation included hemorrhagic transformation. ml/h, P = 0.04), a higher likelihood of parent artery stenosis (65% vs. 20.8%, P < 0.001), and increased need for angioplasty or stenting (50% vs. 17%, P < 0.001). The DWI/ADC volume ratio was calculated by dividing DWI volume by ADC 620 10-6 mm2/s volume.
The PREMIER study first demonstrated high rates of complete occlusion without parent vessel stenosis or permanent neurological complications after the treatment of wide-necked small and medium-sized intracranial ICA aneurysms with the 48-wire pipeline. Median aneurysm and neck size were 5.8 mm (IQR: 4.0-7.5) At a median 10.1 months (IQR: 6.3-12.6),
Only dAVFs with cortical venous drainage were included as this aggressive subtype can present with non‐hemorrhagic neurologic deficits. Additionally, there was a significant association between sinus stenosis and dAVF‐CI (OR: 2.85, 95% CI: 1.16‐7.55, The patients with dAVF‐CI had a mean age of 58 ± 18 years. 7.55, p = 0.027).
Most neurointerventionalists (91%) diagnose ICAS‐LVO after a continued or recurrent occlusion or by the presence of fixed focal stenosis (FFS) after multiple MT attempts. Fear of hemorrhagic complications (70%) was the most compelling reason not to perform RS +/‐ angioplasty. Overall, 40.6%
We tested the Plaque-RADS classification in a cohort of patients with embolic stroke of undetermined source (ESUS) and imaged with neck CTAs.Methods:Patients with unilateral anterior circulation ischemic stroke due to ESUS and neck CTAs showing <50% carotid stenosis were retrospectively identified.
Head CT showed right frontal lobe hemorrhage with bilateral SAHs (Figure1). Brain MRI redemonstrated hemorrhages, numerous scattered foci of restricted diffusion, and a large area of restricted diffusion in the left insular cortex (Figure 2).
One exclusion criterion for tPA administration is stroke within 3 months due to the presumed increased risk of hemorrhage. One study identified 19 patients who received tPA for ERS and found no symptomatic intracranial hemorrhage. While the rate of early recurrent stroke (ERS) within 3 months is as high as 14.5‐18.3%,
Rescue treatment with stenting, balloon angioplasty, and/or intraarterial thrombolysis or antiplatelets are often required to treat the underlying stenosis. Additionally, patients undergoing stenting were less likely to have symptomatic intracranial hemorrhage (sICH) (OR 0.34, 95% CI [0.17 ‐ 0.67]; p = 0.002).
Receiver operating characteristic (ROC) curve analysis was conducted to identify the most accurate CTP parameter for predicting HPP.Results:Forty-six patients were enrolled; four patients exhibited HPP after CAS, and one patient experienced a cerebral hemorrhage.
The ipsilateral cervical ICA was occluded in 11 of 20 patients (55%) and nearly‐occluded (degree of stenosis 90‐99%) in 9 of 20 patients (45%). The degree of cervical ICA stenosis following thrombectomy improved from 96.5% The mean NIHSS was 14 (7‐25) and 40% were treated initially with intravenous thrombolytics.
CT head revealed an evolving acute to subacute right MCA infarction with adjacent small volume subarachnoid hemorrhage. Multifocal severe stenosis was noted in the right distal right M1 and right M2 divisions. CTA head revealed a right MCA bifurcation aneurysm measuring 6 x 6 x 7 mm with irregularity of the wall. mm (Figure 1 ‐A,B).
Inclusion criteria were age ≥18 years, EVT for intracranial occlusion, and underwent treatment for extracranial ICA lesions with >70% stenosis. 5.02; p=0.86), petechial hemorrhages (OR: 0.79, CI: 0.10-6.05; Patients were divided into ASPECTS 0-5 and 6-10 groups. vs 48%, OR: 0.52, CI:0.29-0.97; vs 3.6%, OR: 3.18, CI: 1.07-9.49;
ICAD was present if at least ≥ one of the following features were observed: (1) angiographic evidence of taper‐shape occlusion, (2) presence of arterial calcific lesions, and/or (3) remnant stenosis > 70% after mechanical thrombectomy (MT). There were no symptomatic hemorrhages. mm vs 1.88 ± 0.67 mm, p < 0.01).
Introduction:Current guidelines recommend 24-hours of high-intensity monitoring (HIM) for acute ischemic stroke patients post-intravenous thrombolysis (IVT) due to risk of bleeding complications including symptomatic intracranial hemorrhage (sICH).
History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. 2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. His response: “subendocardial ischemia. Anything more on history? POCUS will be helpful.” Left main? 3-vessel disease?
Patient underwent emergent mechanical thrombectomy with ADAPT to TICI3 revascularization with future plan for possible angioplasty and stenting of R vertebral stenosis. Initially maintained on aspirin and Cangrelor infusion, then transitioned to aspirin and Plavix without hemorrhagic conversion.
Low LV filling pressures are due to several etiologies, most commonly due to volume depletion (dehydration or hemorrhage), but also due to other etiologies including, but not limited to: mitral stenosis, pulmonary hypertension (chronic, or due to pulmonary embolism), or poor RV performance.
Primary outcomes included stroke, intracerebral hemorrhage (ICH), and mortality rates at 1-, 6-, 12-, and 18-month follow-ups, and in-stent restenosis. Multivariable logistic regression identified predictors of stroke and mortality.
Due to the high risk of hemorrhagic conversion, the loading of antiplatelets was deferred. A 2D echocardiogram revealed an ejection fraction of 43%, hypokinesia of the anterior and intraventricular septum from base to apex, and severe mitral stenosis. ml subcutaneously once daily. An open-heart surgery was considered.
Patients with unilateral anterior circulation stroke and <50% carotid stenosis on CTA were retrospectively identified. A semiautomated segmentation software measured intraplaque hemorrhage volumes. Maximum plaque thickness and ulceration were assessed by a neuroradiologist blinded to the stroke side.
We performed this analysis to identify the prevalence of atrial fibrillation and associated outcomes in symptomatic internal carotid artery stenosis patients undergoing CAS or CEA.Methods:We analyzed the data from the National inpatient sample (NIS) between January 2016 to December 2021. versus 18.8% for CAS or CEA, respectively, p=0.50].
There were 4 primary safety events in 4 patients (4.9%, 4/82); 1 nonembolic stroke due to exacerbated cardiac tamponade secondary to catheter perforation and 3 hemorrhagic vascular access complications. Eighty patients (98%) underwent remapping.
Men exhibited more unstable plaques (P<0.001), characterized by increased plaque hemorrhage, larger lipid core, and inflammation (P<0.001), along with less favorable circulating profiles. Adipokine, lipid, and immune profiling was conducted. Plaque stability was determined by gold-standard histological classifications.
61,62) The interventional community defines occlusive LM disease as >50% by FFR, or ≥75% stenosis,(63) but urgent or emergent intervention on lesions not meeting these thresholds is only imperative if it is a thrombotic lesion and the patient has refractory ischemic symptoms (i.e. TIMI 0/1 flow).(61,62) Knotts et al.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content