This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
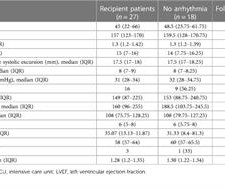
In adults with congenital heart disease (ACHD patients), atrial arrhythmias (AA) and heartfailure (HF) are common. 1 Factors related to congenital heart disease, such as underlying anatomy, surgical repair technique and scars, can all be considered as AA substrates.
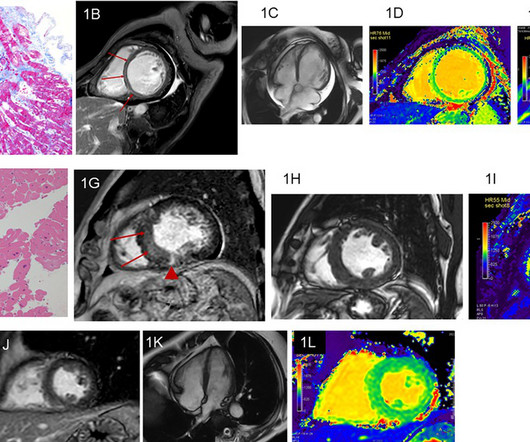
ObjectiveThe aim of this retrospective study was to evaluate the usefulness of non-contrast cardiac magnetic resonance imaging, including cine imaging, T1 and T2 mapping, and texture analysis for T1 mapping, for identifying etiologies of heartfailure (HF).MethodsForty-seven MethodsForty-seven patients with HF were examined using a 1.5T
Then I always look to see if the initial deflection of the QRS has a lot of voltage change per change in time (seen in tachycardias that are initiated from above the ventricle because the propagate through fast conducting purkinje fiber. Tachycardia exaggerates ST Elevation in LBBB and Paced rhythm 5. Pacemaker mediated tachycardia!
So, we can assume the patient was probably being treated for angina, heartfailure, and hypertension. The ECG : The first impression is that is a regular WIDE COMPLEX TACHYCARDIA. It pays to take a moment to consider the possibility of REGULAR REALLY WIDE COMPLEX TACHYCARDIA (RRWCT) before making a treatment decision.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. The heart rate is about 130 bpm. The heart rate could be compatible with that of a 2:1 conducted atrial flutter. The ECG below was recorded. Is this: 1.
Clinical introduction A woman in her 60s with non-obstructive coronary artery disease, aortic valve replacement and aortic arch repair, chronic diastolic heartfailure and paroxysmal atrial fibrillation (AF) and flutter (AFL), presented with 3 days of sustained palpitations that felt similar to prior episodes of AF/AFL.
Permanent pacer placement Later, a biventricular pacer was placed for " Cardiac Resynchronization Therapy (CRT) " (This is indicated for patients with LBBB and QRS duration > 130 ms and heartfailure and vastly improves heartfailure). Even with tachycardia and a paced QRS duration of ~0.16 J Am Coll Cardiol.
Catheter ablation for ventricular tachycardia (VT) has been shown to decrease the risk of VT recurrence and hospitalization. However, a critical gap exists in national-level data assessing its impact on hospital outcomes in patients with acute heartfailure with reduced ejection fraction (HFrEF).
The goals of the current scientific research on ventricular tachycardia (VT) ablation included studies to prove the benefit of early ablation on heartfailure progression and mortality and the need to better characterize and treat heterogeneous deep VT substrates.
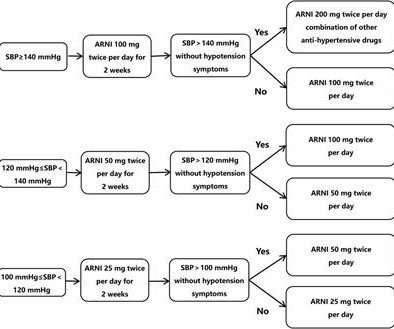
Sacubitril/valsartan can improve outcomes for patients with heartfailure and ventricular tachycardia, but few studies examined whether it can reduce recurrence or improve cardiovascular outcomes in patients with persistent atrial fibrillation after catheter ablation.
Predicting the anticipated benefit and selecting the optimal timing of catheter ablation of recurrent ventricular tachycardia (VT) in patients with severe heartfailure (HF) can be challenging.
Electrical storm (ES) is associated with a high mortality, leads to recurrent hospitalization due to heartfailure or ICD therapy deliveries. Ventricular tachycardia (VT) ablation has demonstrated efficacy in lowering VT recurrences but prompt ablation is challenging and the exact timing still unknown.
Tachycardia-induced cardiomyopathy (TIC) is a unique cardiomyopathy, which is potentially reversible. Investigating miRNA changes in TIC could aid in developing novel therapies and serve as biomarkers, aiming to reduce heartfailure and transplantation burdens.
Cardio-oncology is a new field of interest in cardiology focusing on the detection and treatment of cardiovascular diseases, such as arrhythmias, myocarditis, and heartfailure, as side-effects of chemotherapy and radiotherapy. The association between chemotherapeutic agents and arrhythmias has previously been established.
We present a patient with a history of heartfailure and metallic aortic and mitral valves surgeries, who required ablation for a drug-refractory left ventricular tachycardia. But the metallic valves prohibite.
Ivabradine is an anti-arrhythmic agent that reduces the heart rate through inhibition of the pacemaker current of the sinoatrial node. It has been used to treat both inappropriate sinus tachycardia and sinus tachycardia related to heartfailure in children and adults.
Wild-type transthyretin amyloid cardiomyopathy (ATTRwt-CM) is often accompanied by atrial fibrillation (AF), atrial flutter (AFL), and atrial tachycardia (AT), which are difficult to control because beta-blockers and antiarrhythmic drugs can worsen heartfailure (HF).
A man in his 50s with recurrent palpitations, fatigue, and progressive exertion dyspnea had irregular narrow-QRS tachycardia in an incessant, repetitive fashion with heart rates up to 180 beats per minute and occasional short runs of wide-QRS tachycardia on Holter monitoring and 12-lead electrocardiogram.
She was noted to be in heartfailure, with hypotension and tachycardia. With decompensated heartfailure and adequate prior anticoagulation, the patient underwent direct current synchronised cardioversion for her arrhythmia. Echocardiography demonstrated severe calcific mitral stenosis with pulmonary hypertension.
Louis-based Washington University School of Medicine researchers found radiation therapy can improve outcomes in patients with ventricular tachycardia.
MY Thoughts on this CASE: Not being there — I am unaware of physical exam parameters ( blood pressure, respiratory rate; oxygen saturation; heart and lung auscultation, etc. ). I see the following: There is sinus tachycardia ( upright P wave with fixed PR interval in lead II ) — at the rapid rate of ~130/minute.
Her heart rate was very fast, so we obtained an ECG immediately: ECG: What do you think? There is a regular wide complex tachycardia. Remember : Adenosine is safe in Regular Wide Complex Tachycardia. Rather, from this one: Very Fast Very Wide Complex Tachycardia Ideally, one would cardiovert.
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heart disease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heartfailure for the last five years, and a prior ICD implantation five years ago. What is the rhythm? Smith : Are they P-waves?
The above ECGs show the initiation and continuation of a polymorphic ventricular tachycardia. Polymorphic ventricular tachycardia can be ischemic, catecholaminergic or related to QT prolongation. NT-pro-BNP peaked at 4831, consistent with heartfailure. Below are two ECGs from the telemetry monitoring.
Introduction Heart transplantation (HT) is the only treatment option in children with heartfailure secondary to cardiomyopathies and non-reparable congenital heart diseases. One patient developed a complete AV block during acute rejection at 76 months and received a temporary pacemaker.
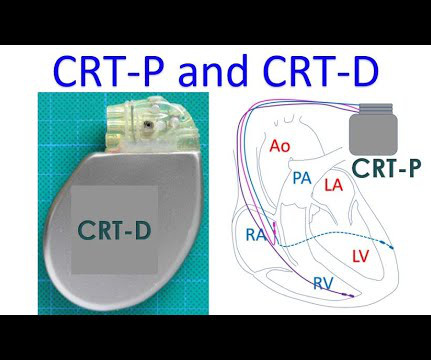
CRT is used in heartfailure with reduced ejection fraction. According to the Universal Definition and Classification of HeartFailure, heartfailure with reduced ejection fraction has left ventricular ejection fraction of 40% or less. CRT stands for cardiac resynchronization therapy.
Patients with anterior LV aneurysm usually have poor LV function and heartfailure. A Closer LOOK at the ECG in Figure-1: The ECG in Figure-1 shows sinus tachycardia — with QRS widening due to complete RBBB. If it is subacute, the first troponin will be elevated, so a rapid troponin can be helpful.
ABSTRACT Atrial flutter (AFL), defined as macro-re-entrant atrial tachycardia, is associated with debilitating symptoms, stroke, heartfailure, and increased mortality. Atypical AFL is a heterogenous group of re-entrant atrial tachycardias that most commonly occur in patients with prior heart surgery or catheter ablation.
Early treatment of persistent AF can reduce the risk of blood clots, stroke, and heartfailure, and may prevent the disease from becoming permanent. Patients are often treated with AADs as frontline therapy for heart rhythm maintenance, though some can experience adverse effects and limited efficacy.
Primary outcome was risk of ischemic stroke while secondary outcomes were all-cause mortality (ACM), heartfailure, acute myocardial infarction (AMI), major adverse cardiovascular events (MACE), atrial fibrillation (AF), and ventricular tachycardia (VT).Result:After 0.46), P<0.01), AMI after 1 year (RR, 0.55(95%CI:
I focus my thoughts on a qualitative approach to these 3 pre-hospital ECGs — all obtained from patients presenting with acute CP ( C hest P ain ). == ECG #1 — from a 70-ish year old Woman with acute CP and Dyspnea The rhythm is sinus tachycardia at a surprisingly rapid rate of ~115/minute.
Arrhythmias : A leadless pacemaker-defibrillator system provides antitachycardia pacing for ventricular tachycardia in patients with subcutaneous ICDs. Coronary Heart Disease : Initiate beta-blockers in patients with acute MI and normal LVEF unless contraindicated or if they have heartfailure.
He was counseled to abstain from cannabis use.Conclusion:At low to moderate doses, cannabis can lead to a surge in sympathetic activity causing tachycardia and hypertension, while parasympathetic activity is predominant at higher doses, causing bradycardia and hypotension. Patient did not report any symptoms and was hemodynamically stable.
But while compressing here in a patient with heartfailure, it can elicit pain because there could be tender hepatomegaly in patients with heartfailure. That occurs in right heartfailure and constrictive pericarditis. One is ventricular tachycardia with regular retrograde activation.
Written by Bobby Nicholson MD, with edits by Meyers A woman in her 50s with past medical history of heartfailure, prior stroke, atrial fibrillation on Eliquis, lung cancer in remission, and CKD, presented to the emergency department for evaluation of cough and shortness of breath. What do you think? References: 1. Khouzam RN.
This is one important cause of supraventricular tachycardia in Ebstein’s anomaly. Ebstein’s anomaly may present with a murmur for evaluation in the pediatric age group or in adults with arrhythmias or heartfailure with cyanosis and exercise intolerance.
Cardioversion is used to correct abnormal heart rhythms, also known as arrhythmias. When your heart beats too quickly, too slow, or irregularly, it can affect your blood flow and lead to severe complications like stroke or heartfailure. Cardioversions can help “reset” your heart rhythm to its regular pattern.
NOTE: It's important to correlate ongoing circumstances at the time that a prior tracing was done ( ie, Was the patient stable and asymptomatic — or were they having chest pain, an exacerbation of heartfailure, or some other ongoing process at the time the prior ECG was recorded? ).
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heartfailure, myocardial infarction, or any prior PCI/stent. Breath sounds were clear in all lung fields. No appreciable skin pallor. He reported to be a social drinker, but used tobacco products daily.
There was a normal creatinine and no evidence of heartfailure and no other reason for chronic injury, so it must be acute. The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis. If it is MI, is it type 1 or type 2? Is it STEMI or NonSTEMI?
For practical purposes — the overwhelming majority of regular SVT rhythms seen in an emergency setting will turn out to be one of the following 4 diagnoses on this LIST: i ) Sinus Tachycardia; ii ) A reentry SVT rhythm ( ie, AVNRT or AVRT ) ; iii ) ATach ( = A trial T achycardia ) ; or , iv ) AFlutter ( A trial F lutter ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content