This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
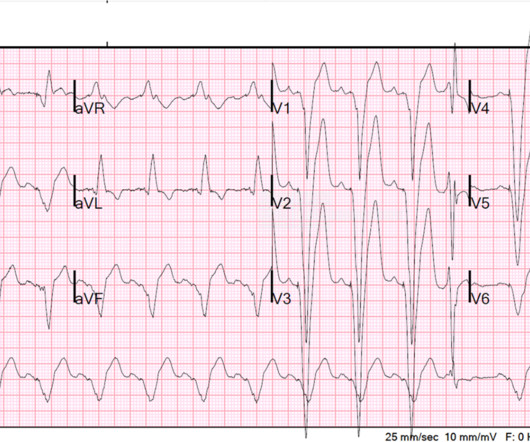
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. He had no h/o heartfailure. Here is the presentation ECG for that inferior STEMI: This looks like a large infarct on ECG. Here is the presentation ECG for that inferior STEMI: This looks like a large infarct on ECG.
His history included known heartfailure with prior EF 18%, insulin dependent diabetes, and polysubstance abuse. Because the most severe LAD OMIs can cause ischemic failure of the RBB and LAF, any patient with ACS symptoms and new RBBB and LAFB with any concordant STE has LAD OMI until proven otherwise.
BACKGROUND:Microvascular obstruction (MVO) is associated with heartfailure (HF) following ST-segmentelevation myocardial infarction. Circulation: Cardiovascular Imaging, Ahead of Print.
That is due to impaired flow through the coronary microcirculation and is associated with higher mortality as well as chance for left ventricular dysunction and heartfailure. Immediate Microvascular Physiology After Mechanical Coronary Reperfusion of STEMI. J Am Coll Cardiol. 2024 May, 83 (21) 2077–2079.
Microvascular resistance reserve (MRR) measured directly after primary PCI was an independent predictor of all-cause mortality or hospitalization for heartfailure (HF) in patients with a STEMI over long-term follow-up, according to the results of a pooled analysis.
Background In acute heartfailure (HF), reduced cardiac output, vasoconstriction and congestion may damage the intestinal mucosa and disrupt its barrier function. Methods We examined 61 ST-elevation myocardial infarction (STEMI) patients who developed acute HF within 48 hours of successful percutaneous coronary intervention (PCI).
Last ECG: Final Diagnosis: "NSTEMI" This patient will likely suffer heartfailure and early death due to the diagnosis of "NSTEMI" Learning Points: Despite NSTEMI guidelines recommending emergent angiography for NSTEMI patients with refractory ischemic symptoms, this is simply not done in many systems, and this has been recorded in a study as well.
Background:The computational pressure-fluid dynamics applied to index of microcirculatory resistance, derived from coronary angiography (CPFD-caIMR) is a promising alternative method of IMR to evaluate the prognosis of STEMI patients. All patients with STEMI underwent CPFD-caIMR and MVO assessment.
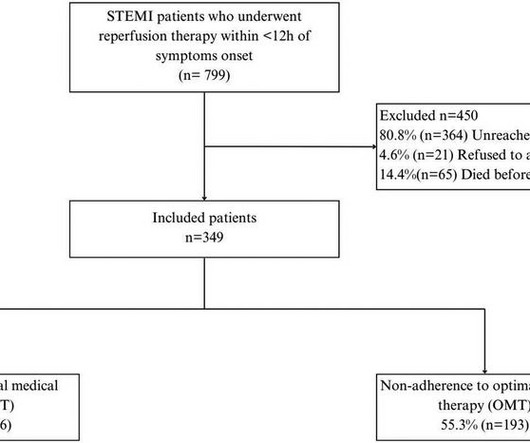
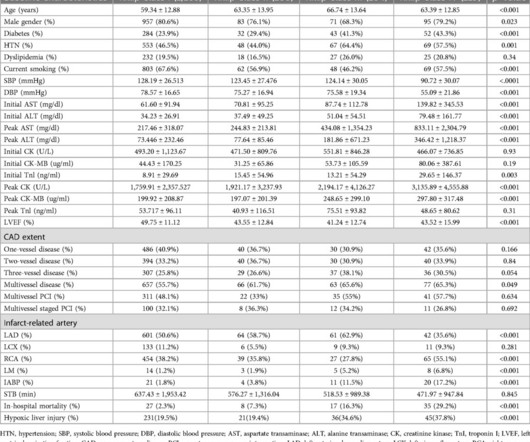
IntroductionIn developing countries, there is a notable scarcity of real-world data on adherence to optimal medical therapy (OMT) and its correlation with major cardiovascular adverse events (MACEs) after ST-elevation myocardial infarction (STEMI). Patients were followed up for 4.5 ResultsWe included 349 patients with a mean age of 58.08
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
Background Hyperglycemia, characterized by elevated blood glucose levels, is frequently observed in patients with acute coronary syndrome, including ST-elevation myocardial infarction (STEMI). There are conflicting sources regarding the relationship between hyperglycemia and outcomes in STEMI patients. 3.45) and 4.47 (95% CI: 2.54–7.87),
Smith comment 2: I frequently see failure to control BP in patients with acute chest pain or acute heartfailure. The Queen of Hearts once again diagnoses OMI with high confidence: The ED provider recognized the changes in this EKG and called cardiology for a STAT consult.
Major adverse cardiovascular events included cardiovascular death, hospitalization for heartfailure, reinfarction, and unplanned revascularization for the target vessel.RESULTS:During a median follow-up of 3.2 MSI was calculated as the ratio of salvageable myocardium to the area at risk. years (interquartile range, 1.64.7
IntroductionHypoxic liver injury (HLI) and Killip classification are poor prognostic factors in patients with ST-segment elevation myocardial infarction (STEMI). Left ventricular ejection fraction (LVEF) was below 45% in symptomatic, overt heartfailure patients (Killip class II, III, and IV).
is very specific for STEMI , and there is some evidence, as well as rationale, that a paced rhythm behaves similarly. Here is one case of anterior STEMI in a paced rhythm. Here is a case of lateral STEMI in a paced rhythm. It is out of proportion to the preceding S-wave, with a maximum ratio in leads V3 and V4 of 10/33 = 0.30.
NH-IMRangiowas calculated based on standard coronary angiographic views with 3-dimensional-modeling and computational analysis of the coronary flow.RESULTS:Overall, ECC (a composite of cardiovascular death, cardiogenic shock, acute heartfailure, life-threatening arrhythmias, resuscitated cardiac arrest, left ventricular thrombus, post-ST-segment–elevation (..)
He has a history of STEMI and heartfailure. link] Case continued The conventional algorithm diagnosed STEMI and so did the paramedics. A Coronary angiogram from 8 years prior revealed that he had had an inferior posterior STEMI at the time due to 100% occlusion of the proximal RCA. He had a prehospital ECG.
BackgroundThere may be variability in willingness to perform percutaneous coronary intervention (PCI) in higherrisk patients who present with STsegmentelevation myocardial infarction (STEMI). There were 178 984 patients from 582 US hospitals presenting with STEMI who were included. versus 7.4%,P<0.001), versus 5.1%,P<0.001)
The outcomes of interest were all-cause death and major adverse cardiovascular events (MACE), including acute coronary syndrome (ACS), heartfailure (HF), need for additional revascularization, target vessel revascularization (TVR), SCAD recurrence, and stroke. Approximately 48.5%
link] In this paper, in a department in which they state they have only 50 STEMI per year, they looked at only 8 days worth of triage ECGs for a total of 538. They did not find one STEMI on their triage ECGs (no surprise! We at HCMC have 30 walk-in STEMIs per year; the rest come by ambulance. Am J Emerg Med 36(10):1771-1774.
Patients with ST-segment elevation myocardial infarction (STEMI) and complex coronary artery disease (CAD) face a poor prognosis, including increased heartfailure (HF) risk. We performed a pooled secondary analysis of 139 patients with STEMI. We performed a pooled secondary analysis of 139 patients with STEMI.
This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. These include: i ) appreciation of how problematic the definition of “acute STEMI” can be; and , ii ) illustration of how dependence on this definition may result in overlooking acute coronary occlusion.
This is documented as a STEMI in the clinical notes and in the cath report, but certainly does not meet STEMI criteria and is therefore an NSTEMI by definition. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0. Large STEMI are approximately 30-80.
This study investigates the relationship between baseline 5-HTP levels and the incidence of major adverse cardiovascular events (MACE) in patients who have experienced ST-elevation myocardial infarction (STEMI).Objective:Our Conclusion:Higher 5-HTP levels are independently associated with a reduced risk of MACE in patients after STEMI.
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heart disease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heartfailure for the last five years, and a prior ICD implantation five years ago. Thus VT is very probable. That was also my initial concern.
The "criteria" for posterior STEMI are 0.5 There was a normal creatinine and no evidence of heartfailure and no other reason for chronic injury, so it must be acute. Is it STEMI or NonSTEMI? The troponin I returned at 4.1 ng/mL (ULN = 0.030 ng/mL) , diagnostic of myocardial injury. mm STE in one lead. This includes: 1.
The patient has heartfailure as a result of this event. Meyers note: notice in their documentation many of the classic mistakes of the STEMI generation: "Non ST Elevation MI" as their reasoning for why the patient did not merit emergent reperfusion, while simultaneously calling it "emergently" (after 8 hours!!!)
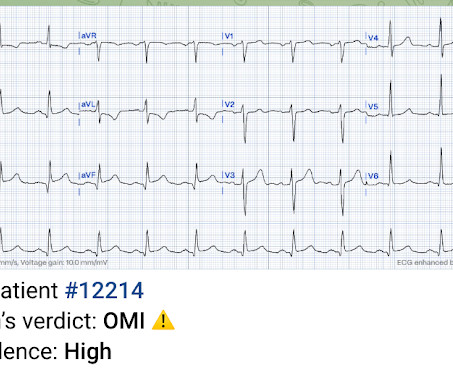
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heartfailure, myocardial infarction, or any prior PCI/stent. It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. No appreciable skin pallor. Is this OMI?
NOTE: It's important to correlate ongoing circumstances at the time that a prior tracing was done ( ie, Was the patient stable and asymptomatic — or were they having chest pain, an exacerbation of heartfailure, or some other ongoing process at the time the prior ECG was recorded? ).
50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. The ECG easily meets STEMI criteria in all leads V2-V6, as well. He was transitioned to oral heartfailure medications and discharged home slightly over one week after presentation.
The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Accordingly, in the algorithm by Cai et al for patients with LBBB and ischemic symptoms ( See below ) — the first indication for PCI is clinical: patients with hemodynamic instability or acute heartfailure.
This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. When OMI is captured in this early phase, there exists the highest amount of salvageable myocardium and least likelihood of heartfailure at hospital discharge. Smith comment : V5 and V6 are excessively discordant!!!!
Explanation: The EKG illustrates an inferior STEMI. The history of failure to revascularize his right coronary artery followed by acute onset heartfailure 48 hours after presentation, as well his examination is most consistent with acute onset mitral regurgitation, secondary to papillary muscle rupture.
The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. Then, three minutes later… Crews activated STEMI as she deteriorated into PEA arrest. A finger-stick glucose resulted 551 mg/dL, and the following ECG was recorded.
It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. As a result — the heart rate of ~115/minute in ECG #1 is a worrisome finding. It suggests a more extensive MI, potentially with resultant heartfailure. The ECG shows ST depression in lead V3.
Higher troponin correlated with more history of heartfailure, diabetes, and hypertension, as well as higher D-dimer, and nearly all inflammatory markers. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease. Median age was 66.4
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. 2 The astute paramedic recognized this possibility and announced a CODE STEMI. Look at the aortic outflow tract. What do you see? Answer below in the still shot.
But lead V2 has a worrisome amount of ST elevation, and in a chest pain patient, I would be worried about STEMI. My subjective interpretation, and that of Pierre's, is of LVH with secondary repolarization abnormalities, including pseudoSTEMI ST elevation in V1-V3. The Ratios of STE to S-wave: V1: 2.5/16
100% occluded RCA with TIMI 0 flow Post drug-eluting stent placement with TIMI 3 flow While in the cath lab, she transiently developed complete heart block and became hypotensive requiring transvenous pacemaker placement and transient pressors. 3) STEMI criteria failed to identify this acute coronary occlusion, like many others.
Does this patient have hypertension and/or heartfailure that has worsened? Clinically it would be important to find out WHAT HAS HAPPENED in the interim between the time that ECG #2 and ECG #1 were done. This might be a common scenario given this patients demographics and his underlying disease ).
Background Women are more likely to develop heartfailure (HF) after myocardial infarction. Methods The patients with PPCI-treated anterior STEMI, from the CIRCUS study cohort, were followed up for 1 year and HF events were recorded. However, diagnosis and reperfusion are often delayed. vs. 4.1%, p = 0.005).
There is worrisome T-wave inversion in inferior leads as well, which is another clue to LAD Occlusion In fact, this ECG meets STEMI criteria!! Why does the conventional algorithm not diagnose STEMI? Transient STEMI, serial ECGs prehospital to hospital, all troponins negative (less than 0.04 Learning Points: 1.
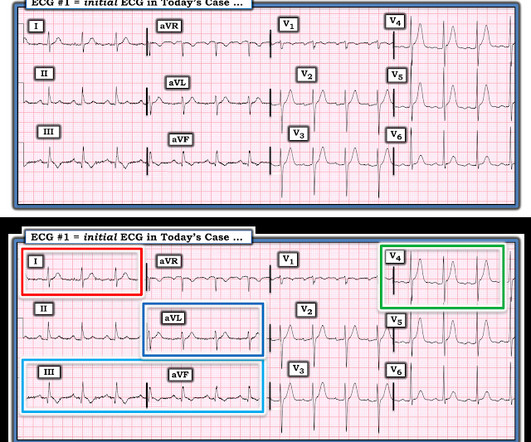
Heres the Queen of Hearts interpretation, drawing attention especially to III and aVL: This patient does indeed need emergent intervention. STEMI criteria are only 43% sensitive for OMI. They end up with high mortality and needless heartfailure. Beware confusing the diagnosis of posterior STEMI by using posterior leads.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content