This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In tricuspid valve regurgitation, a complex condition that Cedars-Sinai experts regularly treat, the valve between two heart chambers on the right side doesn't open or close properly. Makkar explained the advances for patients with tricuspid valve disease in a conversationwith the Cedars-Sinai Newsroom. Image by Getty.
Tricuspid valve disease is an often underrecognized clinical problem that is associated with significant morbidity and mortality. Unfortunately, patients will often present late in their disease course with severe right-sided heartfailure, pulmonary hypertension, and life-limiting symptoms that have few durable treatment options.
Transcript of the video: Ebstein’s Anomaly is one of the cyanotic congenital heart disease in which survival to adult life is common. In Ebstein’s anomaly, there is downward or apical displacement of posterior and septal tricuspid leaflets. Anterior leaflet is elongated and sail like.
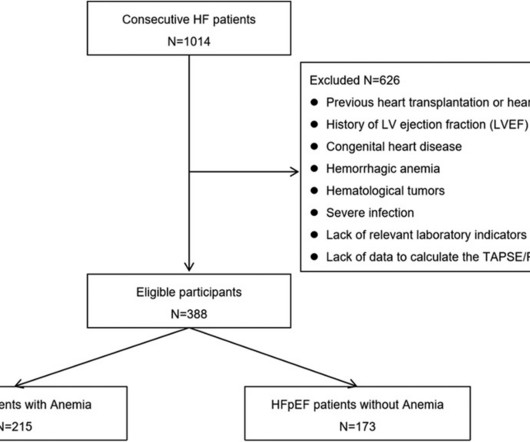
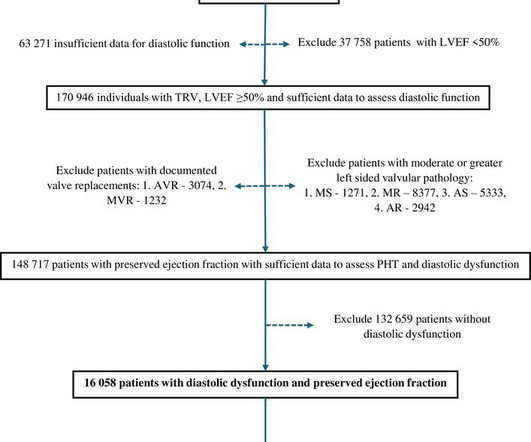
Journal of the American Heart Association, Ahead of Print. BackgroundPulmonary hypertension (PH) is highly prevalent in patients with heartfailure with preserved ejection fraction (HFpEF), and it is a strong predictor of adverse outcomes. TAPSE/PASP and TAS’/PASP can be useful parameters to detect PH in patients with HFpEF.
Prognostic impact of severe tricuspid regurgitation (TR) in patients with atrial functional mitral regurgitation (AFMR). Abstract Aims Tricuspid regurgitation (TR) is often seen in patients with atrial functional mitral regurgitation (AFMR). The primary endpoint was a composite of heartfailure hospitalization and all-cause mortality.
If hemodynamic overload is sustained, it can progress to a maladaptive state and lead eventually to heartfailure. Aims Conventional parameters of right ventricular (RV) function are load-dependent and therefore do not accurately reflect contractility in patients with relevant tricuspid regurgitation (TR).
Objectives Inferior vena cava (IVC) diameter may be a surrogate for volume status in acute decompensated heartfailure (ADHF). IVC diameter correlated to pulmonary arterial (PA) pressure (R=0.347, p<0.001) and body surface area (BSA) (R=0.424 p<0.001). The utility of IVC diameter measurement is under studied.
Introduction Isolated tricuspid valve surgery (TVS) may be associated with high morbidity and mortality. Patients with congenital heart disease, infective endocarditis and those who underwent concomitant valve or pericardial surgery were excluded. The primary outcome was a composite of mortality and congestive heartfailure at 1 year.
ABSTRACT Background Left atrial (LA) myopathy is increasingly recognized as an important phenotypic trait in heartfailure (HF) with preserved ejection fraction (HFpEF). There were 94 patients with events over a median follow-up of 2.9 (IQR 2.92, p = 0.01).
Abstract Aim Functional or secondary tricuspid regurgitation (STR) is the most common phenotype of tricuspid regurgitation (TR) with atrial STR (ASTR) and ventricular STR (VSTR) being recently identified as two distinct entities. ASTR vs. VSTR) are lacking. Patients not matching these criteria were classified as VSTR.
Results Out of 43 (16%) consecutive patients with severe CHD and liver metastases of midgut NETs, 79% presented with right-sided heartfailure. Tricuspid valve replacement was performed in 26 (53%) patients including 19 (73%) cases of combined pulmonary valve replacement.
And that will be the approximate level of the tricuspid valve, the reference point for measuring right atrial pressure. But while compressing here in a patient with heartfailure, it can elicit pain because there could be tender hepatomegaly in patients with heartfailure. X descent, X prime descent and Y descent.
consistent with RAA (which is consistent with this patient’s underlying heart disease. Perhaps the patient has pulmonary hypertension and/or tricuspid regurgitation? Typically — this may be cause by a very “sick” patient (as is the case for your patient) and/or hypoxemia, electrolyte disorders, heartfailure, etc.
Right-sided cardiac damage (rCD) was defined as pulmonary vasculature/tricuspid/right ventricular damage. Hospitalization for heartfailure (HHF) and/or death served as primary endpoint. The extent of cardiac damage was assessed by echocardiography according to an established staging classification.
The primary endpoint was the composite of cardiovascular death and rehospitalisation for heartfailure (HF). Advanced EVCD was defined as pulmonary circulation impairment, severe tricuspid regurgitation or right ventricular dysfunction. CMD was defined as IMR angio ≥30 units.
Some of the other useful parameters are mitral E velocity deceleration time, changes in mitral inflow with Valsalva maneuver, mitral L velocity, isovolumic relaxation time, left atrial maximum volume index, pulmonary vein systolic/diastolic velocity ratio, color M-mode Vp and E/Vp ratio.
CXR confirmed bilateral pulmonary edema and bilateral small effusions. There is mild-moderate tricuspid valve regurgitation. I admitted her to cardiology with these concerns, and we agreed that cardiac MRI may help us confirm possible ARVC. The basal anterior wall and basal septum are hypokinetic. RVEF 34%, RV is mildly enlarged.
Methods Patients with moderate SMR were retrospectively included and stratified by New York Heart Association (NYHA) class and specific aetiology (atrial SMR (aSMR) or ventricular SMR (vSMR)) with a further classification of vSMR based on left ventricular ejection fraction (LVEF) ≥40% or <40%.
Program Designations Access and Publications (A&P) 1 Participant User File (PUF) 2 Task Force on Funded Research (TFR) 3 Special Projects 4 Adult Cardiac Surgery Database Lead Author Title Publication Date William Keeling 2 National Trends in Emergency Coronary Artery Bypass Grafting European Journal of Cardiothoracic Surgery October 2023 Jake (..)
In tricuspid valve regurgitation, a complex condition that Cedars-Sinai experts regularly treat, the valve between two heart chambers on the right side doesn't open or close properly. Makkar explained the advances for patients with tricuspid valve disease in a conversationwith the Cedars-Sinai Newsroom. Image by Getty.
Aims Pulmonary hypertension (PHT) appears to be very common in heartfailure with preserved ejection fraction but details on its prevalence, severity and prognostic implications have not been well defined.
AimsSignificant tricuspid regurgitation (TR) in atrial fibrillation (AF) patients is becoming a global issue, as it can lead to progressive right ventricular enlargement and heartfailure, thereby increasing morbidity and mortality.
AF, atrial fibrillation; LAVI, left atrial volume index; RA, right atrial; RV, right ventricular; sPAP, systolic pulmonary artery pressure; SVI, stroke volume index; TR, tricuspid regurgitation. In addition, the TAPSE/systolic pulmonary artery pressure ratio (TAPSE/sPAP) was monitored as a measure of RVpulmonary arterial (PA) coupling.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content