This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
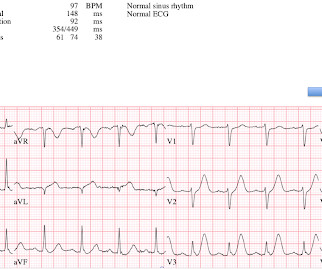
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. He had no h/o heartfailure. The ejection fraction after this infarction was 60%; it had been 70% prior to the infarction. Here is the presentation ECG for that inferior STEMI: This looks like a large infarct on ECG.
Background In acute heartfailure (HF), reduced cardiac output, vasoconstriction and congestion may damage the intestinal mucosa and disrupt its barrier function. We aimed to investigate gut leakage markers and their associations with inflammation, infarct size and cardiac function. to 264.65).
Background Hyperglycemia, characterized by elevated blood glucose levels, is frequently observed in patients with acute coronary syndrome, including ST-elevation myocardialinfarction (STEMI). There are conflicting sources regarding the relationship between hyperglycemia and outcomes in STEMI patients.
IntroductionHypoxic liver injury (HLI) and Killip classification are poor prognostic factors in patients with ST-segment elevation myocardialinfarction (STEMI). Left ventricular ejection fraction (LVEF) was below 45% in symptomatic, overt heartfailure patients (Killip class II, III, and IV).
BACKGROUND:Microvascular obstruction (MVO) is associated with heartfailure (HF) following ST-segmentelevation myocardialinfarction. Circulation: Cardiovascular Imaging, Ahead of Print.
It is now well known that even if a coronary artery is opened well after a myocardialinfarction, with good flow in the epicardial coronary arteries, there could be impaired myocardial perfusion. In the initial era of primary PCI, angiographic myocardial blush was taken as a surrogate of effective myocardial reperfusion.
BackgroundThere may be variability in willingness to perform percutaneous coronary intervention (PCI) in higherrisk patients who present with STsegmentelevation myocardialinfarction (STEMI). There were 178 984 patients from 582 US hospitals presenting with STEMI who were included. versus 7.4%,P<0.001),
The patient has heartfailure as a result of this event. Angiogram: "ACS - Non ST Elevation MyocardialInfarction. This is a HUGE myocardialinfarction. How could an occlusion (Occlusion MI, OMI) that results in the loss of a massive amount of myocardium and results in HeartFailure be missed?
Smith comment 2: I frequently see failure to control BP in patients with acute chest pain or acute heartfailure. The Queen of Hearts once again diagnoses OMI with high confidence: The ED provider recognized the changes in this EKG and called cardiology for a STAT consult. Murakami MM.
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heartfailure, myocardialinfarction, or any prior PCI/stent. It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. No appreciable skin pallor.
ng/mL (ULN = 0.030 ng/mL) , diagnostic of myocardial injury. The "criteria" for posterior STEMI are 0.5 The elevated troponin is diagnostic of myocardial injury. There was a normal creatinine and no evidence of heartfailure and no other reason for chronic injury, so it must be acute. Is it STEMI or NonSTEMI?
The ECG is diagnostic of occlusion myocardialinfarction (OMI). It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. The Queen Of Hearts app is an excellent tool to assist in expediting cardiac cath and emergent revascularization in the cath lab!
This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. When OMI is captured in this early phase, there exists the highest amount of salvageable myocardium and least likelihood of heartfailure at hospital discharge. Smith comment : V5 and V6 are excessively discordant!!!! 40; 1234-1241.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. 2 The astute paramedic recognized this possibility and announced a CODE STEMI. myocardialinfarction), arrhythmias, valvular pathology, shunts, or outflow obstructions.
100% occluded RCA with TIMI 0 flow Post drug-eluting stent placement with TIMI 3 flow While in the cath lab, she transiently developed complete heart block and became hypotensive requiring transvenous pacemaker placement and transient pressors. 3) STEMI criteria failed to identify this acute coronary occlusion, like many others.
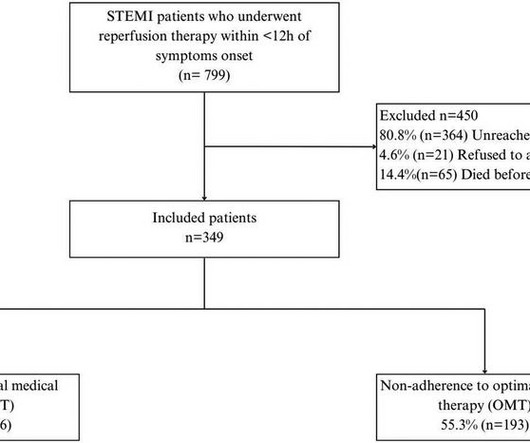
IntroductionIn developing countries, there is a notable scarcity of real-world data on adherence to optimal medical therapy (OMT) and its correlation with major cardiovascular adverse events (MACEs) after ST-elevation myocardialinfarction (STEMI). Patients were followed up for 4.5 years (±10.9), predominantly male (89.9%).
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
Background Women are more likely to develop heartfailure (HF) after myocardialinfarction. Methods The patients with PPCI-treated anterior STEMI, from the CIRCUS study cohort, were followed up for 1 year and HF events were recorded. The infarct size and LVEF were similar between the sexes.
This study investigates the relationship between baseline 5-HTP levels and the incidence of major adverse cardiovascular events (MACE) in patients who have experienced ST-elevation myocardialinfarction (STEMI).Objective:Our years, 53 women) followed for up to 15 years.
Patients with ST-segment elevation myocardialinfarction (STEMI) and complex coronary artery disease (CAD) face a poor prognosis, including increased heartfailure (HF) risk. We performed a pooled secondary analysis of 139 patients with STEMI.
The outcomes of interest were all-cause death and major adverse cardiovascular events (MACE), including acute coronary syndrome (ACS), heartfailure (HF), need for additional revascularization, target vessel revascularization (TVR), SCAD recurrence, and stroke. Approximately 48.5%
BACKGROUND:T2-weighted imaging is commonly used to measure myocardial salvage in reperfused myocardialinfarction but is hindered by poor reproducibility and indistinct boundaries. The median MSI was 35.0% (interquartile range, 22.959.5%), with smaller MSI observed in patients with larger infarcts (P<0.001).
BACKGROUND:Patients with ST-segment–elevation myocardialinfarction but no coronary microvascular injury are at low risk of early cardiovascular complications (ECC). CONCLUSIONS:NH-IMRangiois a valuable risk-stratification tool in patients with ST-segment–elevation myocardialinfarction.
This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. Therefore, this does not meet the definition of myocardialinfarction ( 4th Universal Definition of MI ), which requires at least one troponin above the 99% reference range. No further troponins were drawn. Why is this important?
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. In normal times, the most common use of cTni is in diagnosing, or ruling out, acute myocardialinfarction (AMI, a subcategory of acute myocardial injury.
The utility of the triage electrocardiogram for the detection of ST-segment elevation myocardialinfarction. link] In this paper, in a department in which they state they have only 50 STEMI per year, they looked at only 8 days worth of triage ECGs for a total of 538. They did not find one STEMI on their triage ECGs (no surprise!
There is worrisome T-wave inversion in inferior leads as well, which is another clue to LAD Occlusion In fact, this ECG meets STEMI criteria!! Why does the conventional algorithm not diagnose STEMI? Transient STEMI, serial ECGs prehospital to hospital, all troponins negative (less than 0.04 Learning Points: 1.
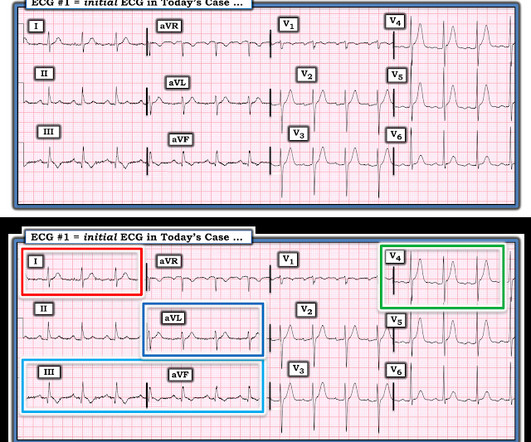
Heres the Queen of Hearts interpretation, drawing attention especially to III and aVL: This patient does indeed need emergent intervention. STEMI criteria are only 43% sensitive for OMI. They end up with high mortality and needless heartfailure. Beware confusing the diagnosis of posterior STEMI by using posterior leads.
Smith: T waves are very hyperacute: these are a sign of ACUTE infarction, even if there are Q-waves. 50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). See Raitt et al.:
The authors describe a case with some features in common with our patient -- a stressful event followed by a stress cardiomyopathy/acute myocardialinfarction overlap syndrome. In addition to profound acute heartfailure, the patient suffered from electrical storm. Journal of the American Heart Association , 8 (9).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content