This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In adults with congenital heartdisease (ACHD patients), atrial arrhythmias (AA) and heart failure (HF) are common. 1 Factors related to congenital heartdisease, such as underlying anatomy, surgical repair technique and scars, can all be considered as AA substrates.
Vitals were normal except for a heart rate of 226. A prehospital 12-lead was recorded: There is a regular wide complex tachycardia. The computer diagnosed this as Ventricular Tachycardia. There is a wide complex regular tachycardia at a rate of 226. It is NOT dangerous when the tachycardia is regular. Pulse is 169.
The goal of the VANISH2 trial was to compare endocardial catheter ablation with conventional antiarrhythmic drug (AAD) therapy as a first-line treatment for infarct-related ventricular tachycardia (VT) in ischemic cardiomyopathy.
A patient in the ICU with significant underlying cardiac disease [HFrEF 30%, non-ischemic cardiomyopathy, LBBB s/p CRT-D (biventricular pacer), AVNRT s/p ablation a few yrs ago, hx sinus tachycardia while on max tolerated BB therapy] went into a regular wide-complex tachycardia after intubation for severe COPD exacerbation.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. The heart rate is about 130 bpm. The heart rate could be compatible with that of a 2:1 conducted atrial flutter. The ECG below was recorded. Is this: 1.
The study enrolled 196 patients randomized 1:1 to ICD vs no ICD and reported a 56% improvement in survival with an ICD in patients with coronary heartdisease, reduced ventricular function, nonsustained ventricular tachycardia (VT), and inducible VT.
What is the feasibility and safety of ventricular tachycardia (VT) ablation in patients with structural heartdisease using a zero-fluoroscopy approach?
If the patient is at least middle-aged , and especially if there is a history of underlying heartdisease then statistical likelihood that a regular WCT without atrial activity will be VT increases to ~90%. ECG Blog #422 and Blog #425 Cases with Congenital HeartDisease in Adults.
Broad complex tachycardia in a 78-year-old patient with coronary heartdisease (CHD) and an old inferior myocardial infarction. Why is this a ventricular tachycardia (VT) and not a supraventricular tachycardia (SVT) with aberrant conduction? What other clues are there?
Ivabradine is an anti-arrhythmic agent that reduces the heart rate through inhibition of the pacemaker current of the sinoatrial node. It has been used to treat both inappropriate sinus tachycardia and sinus tachycardia related to heart failure in children and adults.
On the monitor patient had wide-complex tachycardia. Differential is ventricular tachycardia versus supraventricular tachycardia with aberrancy versus sinus tachycardia with a aberrancy. After the patient was stabilized with supportive care, the heart rate gradually slowed, confirming sinus tachycardia.
Three or more ventricular beats in a row at a rate above 100 per minute is termed ventricular tachycardia. Ventricular tachycardia lasting more 30 seconds or requiring termination earlier due to hemodynamic compromise is called sustained ventricular tachycardia. Either case, the treatment is ablation of the right bundle.
Ventricular tachycardia (VT) with a 1:1 V-His relation can be seen in bundle branch reentry (BBR) or with passive retrograde activation from scar-related VT (SRR-VT) or reentry using left ventricular (LV) Purkinje fascicles (FPVT).
Here was his initial ECG: Regular Wide Complex Tachycardia. Normal 0 false false false EN-US X-NONE X-NONE MicrosoftInternetExplorer4 Approach to Wide Complex Tachycardia Unstable – Shock it 12-lead if at all possible --Unstable defined by : Chest Pain Shock Hypotension Very dyspneic Pulmonary Edema Stable Get a 12-lead ECG Sinus?
Idiopathic fascicular ventricular tachycardia is a unique form of Purkinje-related reentrant monomorphic VT that occurs in the absence of structural heartdisease. Here, we present a case of recurrent ventricular tachycardia.
With this study, we aimed to estimate the prevalence of structural heartdisease (SHD) and decipher the prognostic implications of CMR in selected patients presenting with significant VAs. A change in diagnosis after use of CMR ranged from 21% to 66% with a pooled average of 35% (29%–41%).
Here is her ED ECG: Here is the ED physician's interpretation: IMPRESSION UNCERTAIN REGULAR RHYTHM, wide complex tachycardia, likely p-waves. LEFT BUNDLE BRANCH BLOCK [120+ ms QRS DURATION, 80+ ms Q/S IN V1/V2, 85+ ms R IN I/aVL/V5/V6] Comparison Summary: LBBB and tachycardia are new. This is clearly ventricular tachycardia.
His previous echo one month prior shows the same thing: “consistent with old infarct in LAD vascular territory, with EF 45%” "I think there is something else causing his tachycardia which is exaggerating his EKG findings and mimicking an acute myocardial infarction." The patient spontaneously converted back to sinus tachycardia.
A 28-year-old man with recurrent palpitations and no structural heartdisease presented with a documented wide QRS complex tachycardia (WCT). He had a history of slow pathway ablation for atrioventricular nodal reentrant tachycardia three months ago.
Blood Pressure Many medications used to treat congenital heartdisease can affect blood pressure levels. Heart Rate and Rhythm Some medications can slow down or speed up your heart rate. Your healthcare provider may recommend you wear a heart rate monitor or perform regular pulse checks to monitor your heart rate.
The study provides real-world evidence that a wide range of patients can safely and effectively use the experimental drug, called etripamil, to treat recurrent paroxysmal supraventricular tachycardia (PSVT) episodes at home, potentially sparing them the need for repeated hospital trips for more invasive treatments.
Ventricular Tachycardia (VT) is an important cause of morbidity and mortality in structural heartDisease. Current literature is limited in direct comparison of VT in ischemic (ICM) compared to non-ischemic cardiomyopathy (NICM).
Multiple risk factors for arrhythmia recurrence after Ventricular Tachycardia (VT) ablation have been identified. However, the cumulative impact of these risk factors has not been evaluated, making it challenging to predict these risks in patients with multiple coexisting conditions.
Wide-complex tachycardia: VT or aberrant, or "other?" A wide-complex tachycardia in an older patient must immediately suggest ventricular tachycardia. Sinus tachycardia with aberrancy was unlikely as the rate was consistently 150 bpm, without spontaneous variation. And indeed the QRS morphology strongly supported VT (e.g.
Abstract Introduction Supraventricular tachycardia (SVT) is a common pediatric arrhythmia. Exclusion criteria were pre-excitation, ectopic atrial tachycardia, and hemodynamically significant heartdisease. Methods and Results This is a multicenter retrospective cohort study from three academic children's hospitals.
Congenital heartdisease is a daunting diagnosis for any parent. We’ll cover common types of medications used to treat congenital heartdisease, what parents should know about their use, and potential side effects to watch out for. Be sure to talk to your doctor if you have any questions or concerns.
Initial ECG in the ED: Presenting ECG : Wide-complex tachycardia at a rate about 200. This is overwhelmingly likely to be ventricular tachycardia, even if only age and medical history are considered. Nevertheless, the widths of both the QRS complex and the RS duration are similar in both the old ECG and the tachycardia.
Short-long-short (S-L-S) electrocardiographic cycle length patterns are associated with incidence of ventricular tachycardia (VT) and ventricular fibrillation (VF). It is also recognised that pacemakers can facilitate these cycle length sequences, and that the observation of these sequences can predict future VT/VF events.
Body surface microvolt QRS alternans has been shown to predict ventricular tachycardia (VT) in patients with structural heartdisease, yet its relationship with the VT circuit is undefined.
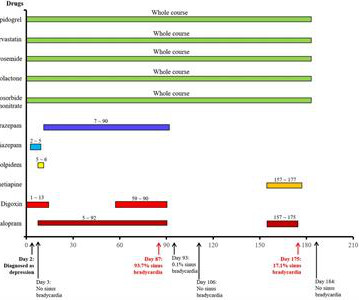
For patients with cardiovascular disease, using the antidepressant escitalopram may lead to unexpected adverse events. In an 82-year-old female patient with cardiac dysfunction using digoxin, tachycardia (average heart rate of 93 beats/min) was demonstrated by electrocardiogram (ECG).
Over the past decade, the care of athletes with a genetic heartdisease (GHD) has been changing with growing support for their return-to-play (RTP). Nevertheless, guidelines surrounding RTP for athletes who are genotype positive but phenotype negative (G+/P-) remain variable and their management challenging.
BACKGROUND:Epicardial approach in ventricular tachycardia (VT) ablation is still regarded as a second-step strategy, due to the risk of complications. Circulation: Arrhythmia and Electrophysiology, Ahead of Print.
Ventricular tachycardia (VT) ablations in patients with structural heartdisease remain challenging procedures with non-trivial rates of acute and short-term complications and VT recurrences, due, in part, to the inherent limitations on size and depth of ventricular lesions produced by existing RF and focal cryo catheters.
All these features together in a cyanotic congenital heartdisease is characteristic of tricuspid atresia. Ebstein’s anomaly may be associated with right sided accessory pathway in ventricular pre-excitation, that is WPW syndrome, with or without atrioventricular re-entrant tachycardia.
C linical I MPRESSION: I would interpret ECG #1 as suggestive of near ventricular standstill — with underlying atrial tachycardia, extended pauses, and no reliable ventricular escape focus. We have no idea how long the pause was before the 1st beat in ECG #1 was recorded. This is often a pre-lethal rhythm.
Monomorphic VT may occur in patients with or without underlying structural heartdisease. The occurrence of monomorphic VT in a patient without underlying structural heartdisease ( and without QT prolongation or metabolic/electrolyte abnormalities ) — is known as Idiopathic VT.
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
A 50-something male with unspecified history of cardiomyopathy presented in diabetic ketoacidosis (without significant hyperkalemia) with a wide complex tachycardia and hypotension. Analysis: there is a wide complex tachycardia. This was the interpretation I put into the system: WIDE COMPLEX TACHYCARDIA. It is regular.
Different imaging modalities have been used to image and display scar tissue accelerating substrate identification and streamlining mapping and ablation of ventricular tachycardias (VTs). Ventricular arrhythmias typically originate from scar tissue.
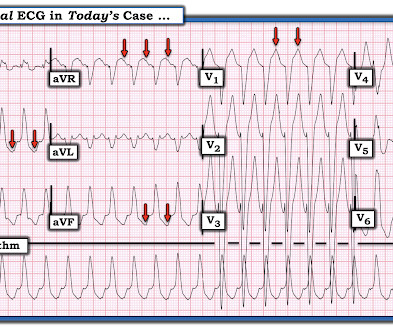
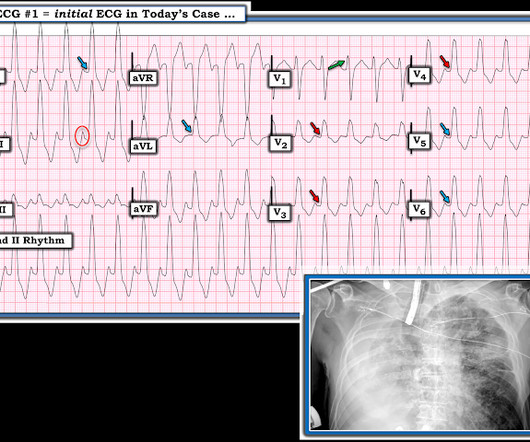
The ECG in Figure-1 was obtained from a young man with a history of rheumatic heartdisease — who presented with “palpitations”. Statistically, in an unselected adult population — VT is much more common than an SVT rhythm , especially in a patient such as the one in today’s case who has underlying heartdisease.
Her clinical tachycardia was easily inducible and had a cycle length (TCL) of 340 ms. A 37-year-old woman with biventricular repair for pulmonary atresia and an intact ventricular septum was referred for an electrophysiological study in the context of recurrent atrial arrhythmias with multiple electrical cardioversions.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content