This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Tetralogy of Fallot TOF with pulmonary atresia Pulmonary atresia with intact interventricular septum Tricuspid atresia Double outlet right ventricle Transposition of great arteries with ventricular septal defect and pulmonarystenosis Ebstein’s anomaly of tricuspid valve In DORV and tricuspid atresia, there are also variants with increased pulmonary (..)
D-Transposition of great arteries Double outlet right ventricle without pulmonarypulmonarystenosis Taussig-Bing anomaly Total anomalous pulmonary venous return Truncus arteriosus Single ventricle (double inlet ventricle, univentricular heart)
Such a pattern is consistent with significant left main coronary artery stenosis. Clinical evaluation and X-Ray chest showed features of pulmonary edema. Angiography done after initial stabilization showed severe stenosis of distal left main coronary artery. ST segment elevation is noted in aVR.
SCAPE is an acronym for sympathetic crash acute pulmonary edema, which can typcially occur in Pickering syndrome with renal artery stenosis [1]. Another term for transient acute pulmonary edema which occurs in renal artery stenosis is flash pulmonary edema. Sympathetic crashing acute pulmonary edem a.
That is, right ventricle is connecting to aorta, and left ventricle to pulmonary artery. That is, pulmonary artery is transposed over to the right ventricle, and aorta over to the left ventricle, so that normal anatomy is restored. In dextro transposition of great arteries or D-TGA, there is ventriculoarterial discordance.
One is ventricular septal defect, second is overriding aorta, third is pulmonarystenosis, usually right ventricular outflow tract stenosis and associated right ventricular hypertrophy. Pulmonarystenosis, which is usually right ventricular outflow tract stenosis. As the name implies, there are four defects.
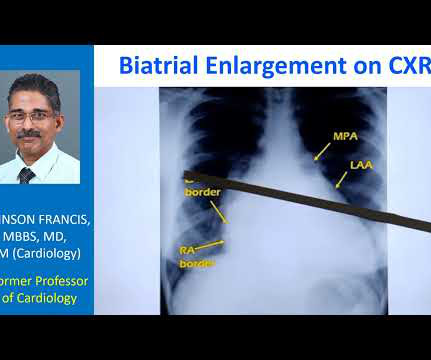
Normally, the main pulmonary artery segment will be concave and left atrial appendage region also will be not prominent. So that is why we see straightening of left border, typically heard of in mitral stenosis with left atrial enlargement and mild pulmonary hypertension. Those are not very clear in this picture.
Sudden breathlessness at night in those with known heart disease is usually due to collection of fluid in the lungs (pulmonary edema). During day time, when one is walking about, any extra fluid in the body tends to collect in the legs, due to the effect of gravity.
Most popular method is pulmonary vein isolation using these energy sources as the pulmonary veins harbour the triggers for atrial fibrillation. Destabilization of cell membranes cause cellular necrosis without any significant heat generation.
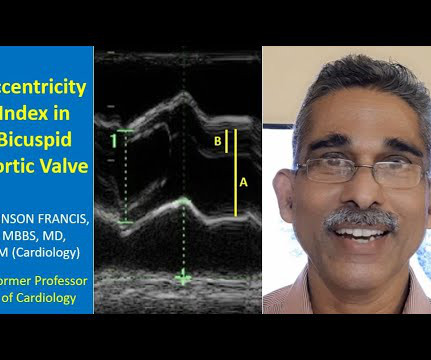
Systole is identified here by the pulmonary arterial colour flow mapping. Bicuspid leaflets are likely to have both stenosis and regurgitation and both can progress as age advances, so that they may present with aortic stenosis most often in the older age group. So you will hardly able to see in real systole.
So it will not produce a true LV to aorta pullback tracing, which is required in cases like aortic stenosis. While standard pigtail catheter is mainly used on the left side, Grollman PA is a catheter used for pulmonary angiography, on the right side. When the tip is in the left ventricle, this region will be in the aorta sometimes.
The Y descent is shallow in tricuspid stenosis, and absent in cardiac tamponade. Right atrial hypertrophy as in tricuspid stenosis, pulmonarystenosis and pulmonary hypertension. But in a VSD with pulmonary hypertension A wave is not prominent. X descent, X prime descent and Y descent.
The aorta, right ventricular outflow tract and pulmonary artery up to its bifurcation is imaged in the upward angulation shown in the left panel. Colour flow shows the flow in pulmonary artery. Planimetry of mitral valve area can be obtained in parasternal short axis view in case of mitral stenosis.
If a nominal right atrial pressure of 10 mm Hg is added to it, right ventricular pressure and indirectly the pulmonary artery systolic pressure are obtained, in the absence of pulmonarystenosis. The early diastolic pulmonary regurgitation (PR) gradient (peak PR gradient) will give an estimate of mean pulmonary artery pressure.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content