This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Pulmonary blood flow is designated as QP and systemic blood flow as QS in hemodynamic calculations. When there is a left to right shunt, pulmonary blood flow is more than the systemic blood flow. The systemic blood flow is more than the pulmonary blood flow when there is a right to left shunt.
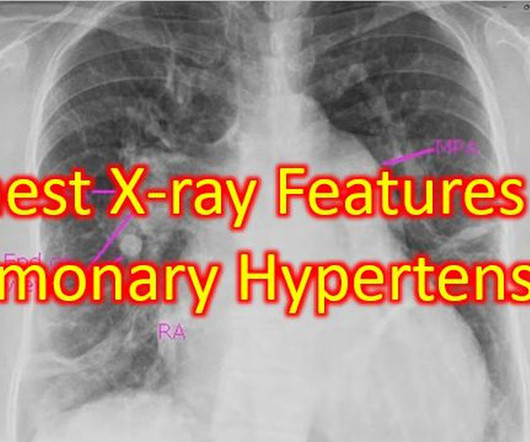
Couple of chest X-rays showing serial changes in pulmonary hypertension over the years and another with features of severe pulmonary hypertension. The post Chest X-ray Features of Pulmonary Hypertension appeared first on All About Cardiovascular System and Disorders.
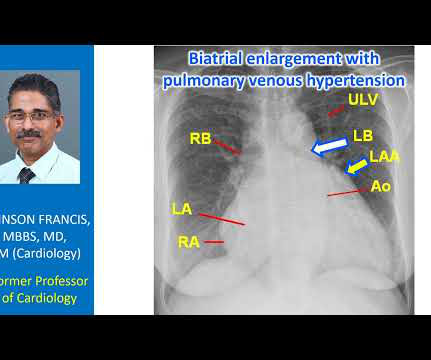
Transcript of the video: Now we will discuss a chest X-ray showing antler sign in pulmonary venous hypertension. So, the shape of the upper lobe vessels in venous hypertension, pulmonary venous hypertension, will be resembling the antlers of the stag. For a change, first we will see the picture of a stag, with antlers.
Tetralogy of Fallot TOF with pulmonary atresia Pulmonary atresia with intact interventricular septum Tricuspid atresia Double outlet right ventricle Transposition of great arteries with ventricular septal defect and pulmonary stenosis Ebstein’s anomaly of tricuspid valve In DORV and tricuspid atresia, there are also variants with increased pulmonary (..)
D-Transposition of great arteries Double outlet right ventricle without pulmonarypulmonary stenosis Taussig-Bing anomaly Total anomalous pulmonary venous return Truncus arteriosus Single ventricle (double inlet ventricle, univentricular heart)
Transcript of the video: Hemodynamic vise is the term given to compression of a vertical vein, which ascends to the brachiocephalic vein, between a bronchus and pulmonary artery. This is the typical location of the hemodynamic vise, between the pulmonary artery and left bronchus. Hence it is known as hemodynamic vise.
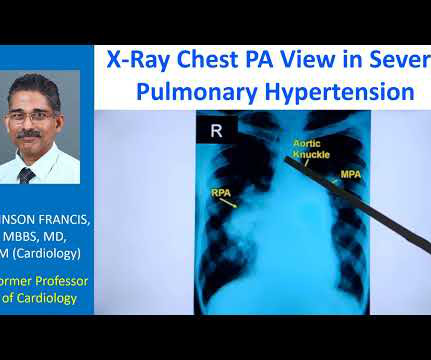
The striking finding is the huge enlargement of the right pulmonary artery, almost aneurysmal dilatation of right pulmonary artery. Main pulmonary artery is also grossly dilated. And you can see left pulmonary artery shadow and rest of it is not seen here. So massive enlargement of pulmonary arteries.
SCAPE is an acronym for sympathetic crash acute pulmonary edema, which can typcially occur in Pickering syndrome with renal artery stenosis [1]. Another term for transient acute pulmonary edema which occurs in renal artery stenosis is flash pulmonary edema. Sympathetic crashing acute pulmonary edem a. Prog Cardiovasc Dis.
As the aorta is small in hypoplastic left heart syndrome, proximal portion of the pulmonary artery is taken and along with the valve, it is used to reconstruct the proximal aorta, this region, and it is connected to the right ventricle. So right ventricle maintains both systemic and pulmonary circulation after a Norwood procedure.
One is ventricular septal defect, second is overriding aorta, third is pulmonary stenosis, usually right ventricular outflow tract stenosis and associated right ventricular hypertrophy. Pulmonary stenosis, which is usually right ventricular outflow tract stenosis. This will almost invariably result in severe pulmonary regurgitation.
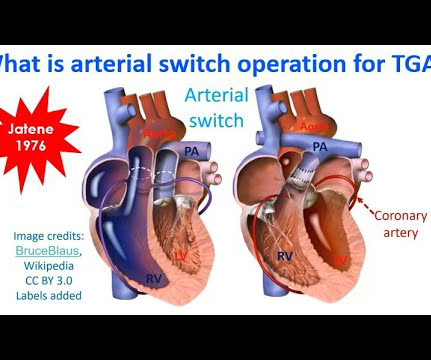
That is, right ventricle is connecting to aorta, and left ventricle to pulmonary artery. That is, pulmonary artery is transposed over to the right ventricle, and aorta over to the left ventricle, so that normal anatomy is restored. In dextro transposition of great arteries or D-TGA, there is ventriculoarterial discordance.
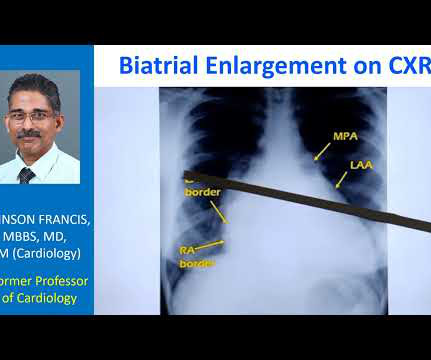
Normally, the main pulmonary artery segment will be concave and left atrial appendage region also will be not prominent. So that is why we see straightening of left border, typically heard of in mitral stenosis with left atrial enlargement and mild pulmonary hypertension. Those are not very clear in this picture.
Transcript of the video: Eisenmenger syndrome is an important complication of large left to right shunts which develop later due to development of pulmonary vascular obstructive disease and severe pulmonary hypertension. So in ASD Eisemenger, suprasystemic pulmonary hypertension is possible. But, leave that alone.
This is the schematic diagram of the heart in which you can see right atrium, right ventricle, left atrium, left ventricle, aorta and pulmonary artery. Similarly, another right sided valve is the pulmonary valve. There could also be some mild leak in the pulmonary valve, both these, in normal persons.
Some of the other useful parameters are mitral E velocity deceleration time, changes in mitral inflow with Valsalva maneuver, mitral L velocity, isovolumic relaxation time, left atrial maximum volume index, pulmonary vein systolic/diastolic velocity ratio, color M-mode Vp and E/Vp ratio.
The severe restriction causes elevation of pulmonary and systemic venous pressure which becomes equal to diastolic pressures in all cardiac chambers. Inspiratory fall in intrathoracic pressure is transmitted to the pulmonary veins, but not to the pericardial cavity. Relative change is more on the right sided chambers.
Most popular method is pulmonary vein isolation using these energy sources as the pulmonary veins harbour the triggers for atrial fibrillation. Destabilization of cell membranes cause cellular necrosis without any significant heat generation.
And if it is more than 50% towards the right side, then you think of another condition known as double outlet right ventricle, where both great vessels, aorta and pulmonary artery arises from the right ventricle. You require multiple views to see from where the pulmonary arteries are arising.
Sudden breathlessness at night in those with known heart disease is usually due to collection of fluid in the lungs (pulmonary edema). During day time, when one is walking about, any extra fluid in the body tends to collect in the legs, due to the effect of gravity.
Leaving a fenestration in the interatrial septum during a Fontan repair is useful in relieving the central venous congestion when pulmonary blood flow is driven by venous pressure in Fontan repair. They noted that benefit was more pronounced if mean pulmonary arterial pressure was 13 mm Hg or more, as expected.
While standard pigtail catheter is mainly used on the left side, Grollman PA is a catheter used for pulmonary angiography, on the right side. It is used for pulmonary angiography by the transfemoral route and it is also used for clot lysis in pulmonary embolism. So it is used both diagnostically as well as therapeutically.
Pulmonary embolism is obstruction of blood vessels of the lungs by clots carried by blood circulation, usually from the legs. Remember that by preventing blood clots in the legs, you are preventing a life threatening disease called pulmonary embolism, in which oxygen level of blood can fall markedly.
Right atrial hypertrophy as in tricuspid stenosis, pulmonary stenosis and pulmonary hypertension. But in a VSD with pulmonary hypertension A wave is not prominent. We noted that prominent V waves or CV waves can occur in tricupsid regurgitation. A prominent A wave can occur when the atrium is hypertrophied.
Systole is identified here by the pulmonary arterial colour flow mapping. This is parasternal short axis view, In normal valve, you can hardly see the leaflets because they are open and almost approximate to the aortic wall. So you will hardly able to see in real systole. This is the corresponding echocardiogram in bicuspid aortic valve.
The cyanosis in Ebstein’s anomaly, is usually not due to pulmonary hypertension, but because tricuspid regurgitation jet is directed across the atrial septal defect. Ebstein’s anomaly may be associated with atrial septal defect or a patent foramen ovale, in about 50% of cases.
Clinical evaluation and X-Ray chest showed features of pulmonary edema. ST segment elevation is noted in aVR. Such a pattern is consistent with significant left main coronary artery stenosis. Angiography done after initial stabilization showed severe stenosis of distal left main coronary artery.
They include myocardial ischemia, acute pericarditis, pulmonary embolism, external compression due to mass over the right ventricular outflow tract region, and metabolic disorders like hyper or hypokalemia and hypercalcemia. These are the conditions which have to be considered or excluded as they can sometimes manifest Brugada pattern on ECG.
The aorta, right ventricular outflow tract and pulmonary artery up to its bifurcation is imaged in the upward angulation shown in the left panel. Colour flow shows the flow in pulmonary artery. Three cuts are usually obtained in this view.
CABANA Trial randomized 2204 patients with AF aged 65 years or more and those below 65 years with one or more risk factors for stroke for catheter ablation with pulmonary vein ablation or drug therapy with rate or rhythm control. Among the subjects of CABANA trial 35% had NYHA class above II at baseline.
If a nominal right atrial pressure of 10 mm Hg is added to it, right ventricular pressure and indirectly the pulmonary artery systolic pressure are obtained, in the absence of pulmonary stenosis. The early diastolic pulmonary regurgitation (PR) gradient (peak PR gradient) will give an estimate of mean pulmonary artery pressure.
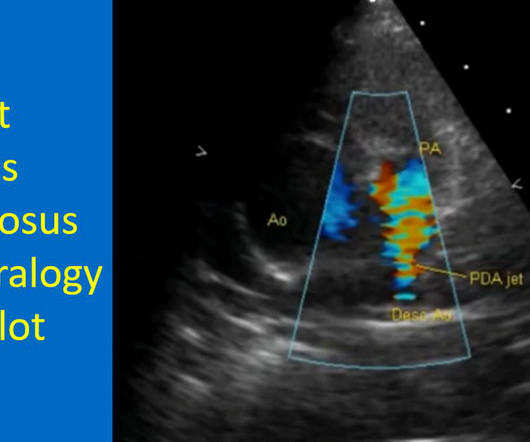
Patent ductus arteriosus in Tetralogy of Fallot, seen as a mosaic colour jet in pulmonary artery. Colour flow imaging shows high velocity jet in the pulmonary artery arising distally, from the descending aorta, suggesting a patent ductus arteriosus (PDA). Intra pulmonary collaterals can also occur in Tetralogy of Fallot.
I has to be done quite early in life before the left ventricular muscle mass regressed due to the lower load of the pulmonary circulation. Rare long term problems include narrowing of the pulmonary artery and aortic regurgitation due to aortic root enlargement. Delayed surgery has been undertaken with ECMO support in some cases.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content