This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
About a fifth of all ischemic strokes are attributed to embolization of ruptured atherosclerotic plaque from carotid arterial stenosis. But it has been difficult to predict which person with asymptomatic carotid artery stenosis is likely to progress to symptomatic carotid disease and stroke. J Am Coll Cardiol. doi: 10.1016/j.jacc.2024.03.389.
One is ventricular septal defect, second is overriding aorta, third is pulmonary stenosis, usually right ventricular outflow tract stenosis and associated right ventricular hypertrophy. Pulmonary stenosis, which is usually right ventricular outflow tract stenosis. As the name implies, there are four defects.
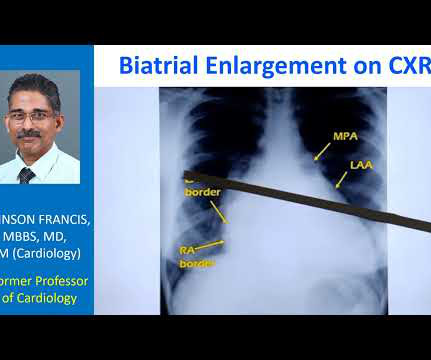
So that is why we see straightening of left border, typically heard of in mitral stenosis with left atrial enlargement and mild pulmonary hypertension. When there is gross pulmonary hypertension, instead of these being straight over here, it will form a bulge over here.
The Y descent is shallow in tricuspid stenosis, and absent in cardiac tamponade. Right atrial hypertrophy as in tricuspid stenosis, pulmonary stenosis and pulmonary hypertension. But in a VSD with pulmonary hypertension A wave is not prominent. X descent, X prime descent and Y descent.
If a nominal right atrial pressure of 10 mm Hg is added to it, right ventricular pressure and indirectly the pulmonary artery systolic pressure are obtained, in the absence of pulmonary stenosis. If there is high right atrial pressure with elevated jugular venous pressure, 15 or 20 mm Hg may have to be added instead of 10 mm Hg.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









Let's personalize your content