This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
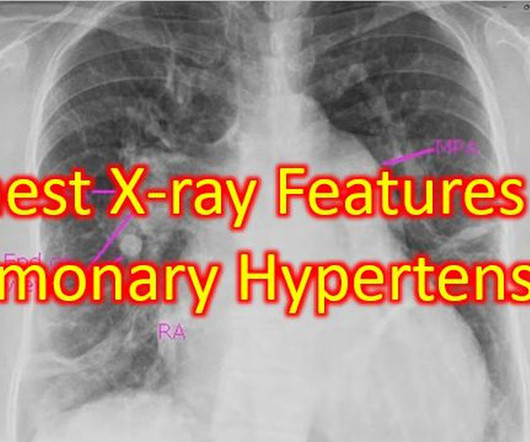
Couple of chest X-rays showing serial changes in pulmonaryhypertension over the years and another with features of severe pulmonaryhypertension. The post Chest X-ray Features of PulmonaryHypertension appeared first on All About Cardiovascular System and Disorders.
Transcript of the video: Now we will discuss a chest X-ray showing antler sign in pulmonary venous hypertension. So, the shape of the upper lobe vessels in venous hypertension, pulmonary venous hypertension, will be resembling the antlers of the stag. You can see the antlers here.
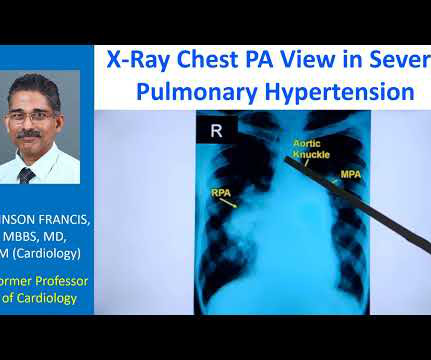
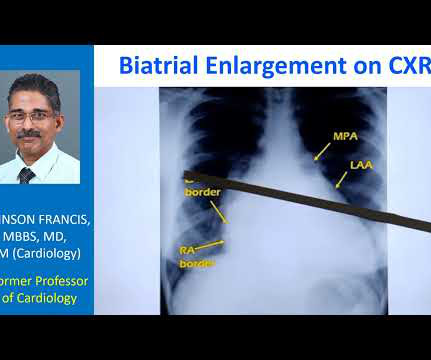
The striking finding is the huge enlargement of the right pulmonary artery, almost aneurysmal dilatation of right pulmonary artery. Main pulmonary artery is also grossly dilated. And you can see left pulmonary artery shadow and rest of it is not seen here. So massive enlargement of pulmonary arteries.
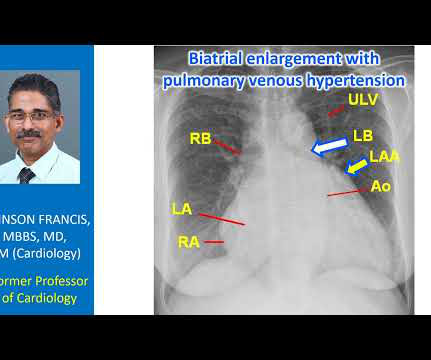
Normally, the main pulmonary artery segment will be concave and left atrial appendage region also will be not prominent. So that is why we see straightening of left border, typically heard of in mitral stenosis with left atrial enlargement and mild pulmonaryhypertension. Those are not very clear in this picture.
Transcript of the video: Eisenmenger syndrome is an important complication of large left to right shunts which develop later due to development of pulmonary vascular obstructive disease and severe pulmonaryhypertension. So in ASD Eisemenger, suprasystemic pulmonaryhypertension is possible. But, leave that alone.
One is ventricular septal defect, second is overriding aorta, third is pulmonary stenosis, usually right ventricular outflow tract stenosis and associated right ventricular hypertrophy. Pulmonary stenosis, which is usually right ventricular outflow tract stenosis. This will almost invariably result in severe pulmonary regurgitation.
Some of the other useful parameters are mitral E velocity deceleration time, changes in mitral inflow with Valsalva maneuver, mitral L velocity, isovolumic relaxation time, left atrial maximum volume index, pulmonary vein systolic/diastolic velocity ratio, color M-mode Vp and E/Vp ratio.
Right atrial hypertrophy as in tricuspid stenosis, pulmonary stenosis and pulmonaryhypertension. But in a VSD with pulmonaryhypertension A wave is not prominent. We noted that prominent V waves or CV waves can occur in tricupsid regurgitation. A prominent A wave can occur when the atrium is hypertrophied.
The cyanosis in Ebstein’s anomaly, is usually not due to pulmonaryhypertension, but because tricuspid regurgitation jet is directed across the atrial septal defect. Ebstein’s anomaly may be associated with atrial septal defect or a patent foramen ovale, in about 50% of cases.
CABANA Trial randomized 2204 patients with AF aged 65 years or more and those below 65 years with one or more risk factors for stroke for catheter ablation with pulmonary vein ablation or drug therapy with rate or rhythm control. Among the subjects of CABANA trial 35% had NYHA class above II at baseline.
If a nominal right atrial pressure of 10 mm Hg is added to it, right ventricular pressure and indirectly the pulmonary artery systolic pressure are obtained, in the absence of pulmonary stenosis. The early diastolic pulmonary regurgitation (PR) gradient (peak PR gradient) will give an estimate of mean pulmonary artery pressure.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












Let's personalize your content