This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BACKGROUND:Prior clinical trials have demonstrated the efficacy of ultrasound-facilitated catheter-directed thrombolysis (USCDT) for the treatment of acute intermediate-risk pulmonary embolism (PE) using reduced thrombolytic doses and shorter infusion durations. Circulation: Cardiovascular Interventions, Ahead of Print.
This Best Case Ever elucidates the practical challenges of working up pregnant patients in the ED with a suspicion of pulmonary embolism. Since this recording, the first ever multi-center prospective outcome study looking at the pulmonary embolism workup in pregnancy was published in the Annals of Internal Medicine.
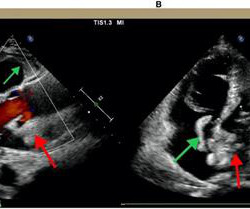
Notably, acute massive pulmonary embolism (PE) with bilateral atrial thrombosis is an exceptional occurrence in CAPS. Acute pulmonary embolism (PE) is a common cardiovascular disease that progresses rapidly and has a high mortality rate. It primarily affects small vessels, seldom impacting large vessels.
The risk factors for postoperative embolism included Black race, interstitial fibrosis, advanced-stage disease requiring bilobectomy or pneumonectomy, and increased operative duration. By increasing awareness of the increased risk for VTE in Black patients, the team hopes to encourage more focused preventative measures in these patients.”
Genetic protein S (PS) deficiency caused by PROS1 gene mutation is an important risk factor for hereditary thrombophilia.Case introductionIn this case, we report a 28-year-old male patient who developed a severe pulmonary embolism during his visit. Ultrasound showed no thrombosis in the veins of both lower limbs.
In patients with narrow QRS ( not this patient), this pattern is highly suggestive of acute pulmonary embolism. Answer : Bedside ultrasound! Smith : RV infarct may also have this appearance on ultrasound. So hypoxia without B lines on lung ultrasound strongly weights toward PE. So CT is required to find the diagnosis!
We have seen this pattern in many pts with acute right heart strain on this blog. __ Smith : The combination of T-wave inversion in V1-V3 and in lead III is very specific for acute pulmonary embolism. Acute pulmonary embolism was confirmed on CT: The patient did well with treatment. Now another, with ultrasound. This is a quiz.
A pathological classification of no-reflow was proposed: structural no-reflow—microvessels within the necrotic myocardium exhibit loss of capillary integrity (it is usually irreversible)—and functional no reflow—patency of microvasculature is compromised due to distal embolization, spasm, ischemic injury, reperfusion injury.
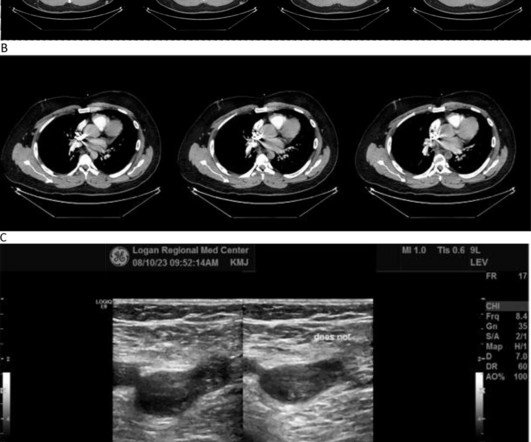
A venous Doppler ultrasound revealed an extensive right lower extremity DVT. Further imaging with a computed tomography (CT) pulmonary embolism (PE) protocol scan of the chest and abdomen identified IVC agenesis along with pulmonary emboli in the left central pulmonary arteries.
Bedside cardiac ultrasound showed moderately decreased LV function. CT of the chest showed no pulmonary embolism but bibasilar infiltrates. (And of course Ken's comments at the bottom) An elderly obese woman with cardiomyopathy, Left bundle branch block, and chronic hypercapnea presented hypoxic with altered mental status.
male with pertinent past medical history including Atrial fibrillation, atrial flutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Bedside ultrasound showed volume depletion and no pulmonary edema.
The post EM Quick Hits 33 Polytrauma Tips & Tricks, Toxic Megacolon, ECG in PE, Patch Calls, CT Before LP, Nebulized Ketamine appeared first on Emergency Medicine Cases.
Rob always wished he had x-ray vision…but since he possesses no special powers…using Point-of-Care Ultrasound (POCUS) is the next closest thing. Robert Simard, an Emergency Physician at North York General Hospital and Sunnybrook Health Sciences Centre in Toronto.
She elected to undergo right MEV coil embolization. Under ultrasound guidance, her PT disappeared when the posterior auricular vein collapsed under applied pressure and returned when the pressure was released. The 3 individuals who have undergone coil embolization of anomalous venous structures have experienced resolution of PT.
Ken (below) is appropriately worried about pulmonary embolism from the ECG. What I had not told him before he made that judgement is that the patient also had ultrasound B-lines of pulmonary edema. I was told that the Queen of Hearts had called it OMI with high confidence. What do you think?
Smith comment: before reading anything else, this case screamed pulmonary embolism to me. I would do bedside ultrasound to look at the RV, look for B lines as a cause of hypoxia (which would support OMI, and argue against PE), and if any doubt persists, a rapid CT pulmonary angiogram.
ET Main Tent (Hall B1) Coronary Sinus Reducer for the Treatment of Refractory Angina: A Randomised, Placebo-controlled Trial (ORBITA-COSMIC) Transcatheter Aortic Valve Implantation Versus Surgical Aortic Valve Replacement in Patients at Low to Intermediate Risk: One Year Outcomes of the Randomized DEDICATE-DZHK6 Trial Effect of Alcohol-mediated Renal (..)
My opinion was that it was not a cath lab case, but I did suggest they do a bedside ultrasound to look for an anterior wall motion abnormality. The RV was small and IVC empty, making pulmonary embolism extremely unlikely. The RV was small and IVC empty, making pulmonary embolism extremely unlikely.
Once stabilized, intravascular ultrasound showed significant thrombus and plaque in the LAD. Due to ongoing shock despite initial mechanical support, the patient was escalated to an Impella CP device after a transthoracic echo confirmed no left ventricle thrombus. This was treated with a drug-eluting stent, but TIMI 3 flow was not achieved.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction.
The problem is difficult to study because angiographic visualization of arteries is not perfect, and not all angiograms employ intravascular ultrasound (IVUS) to assess for unseen plaque or for plaque whose rupture and ulceration cannot be seen on angiogram. Thus, intracoronary imaging modalities are crucial in this setting.
The ways to tell for certain include intravascular ultrasound (to look for extra-luminal plaque with rupture) or "optical coherence tomography," something I am entirely unfamiliar with. pulmonary embolism, sepsis, etc.), Coronary thrombosis or embolism can result in MINOCA, either with or without a hypercoagulable state.
Here is the cardiac ultrasound: The orange colored area is the Definity contrast in the chambers of the heart. This is known as McConnell's sign, and is described for Pulmonary Embolism ; here we see it in right ventricular MI. The RV is on the left (circled below). This shows very poor RV function except at the apex (arrow below).
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. Takotsubo is a sudden event, not one with crescendo angina.
Coronary artery embolism – In this scenario, a blood clot which forms elsewhere goes down a coronary artery, causing a blockage but by the time we do the angiogram, the clot has dissipated and we see unobstructed vessels. myocarditis), and blood clotting disorders.
Patients with pulmonary embolism or aortic dissection who have normal variant ST elevation are at high risk of being diagnosed with pericarditis when what they have is far more serious!! Beware a negative Bedside ultrasound. You diagnose pericarditis at your peril! Acute MI is frequently misdiagnosed as pericarditis. Pericarditis?
He was started on a heparin drip and CTA of the chest was ordered to rule out pulmonary embolism. This is a case like many others posted (see list below) and the EKG from the patient’s original presentation can be quickly recognized as diagnostic for pulmonary embolism. Now another, with ultrasound. In fact, Kosuge et al.
He was requiring supplemental oxygen and an initial bedside cardiac ultrasound was unremarkable. Despite his large clot burden, there was absence of obstructive shock.Transthoracic Echocardiogram and bilateral duplex venous ultrasound were obtained to evaluate for right heart strain and clot burden. Cardiology was consulted.
A bedside cardiac ultrasound was recorded: Here is a still image of the echo: The red arrows outline the right ventricle and the yellow arrows outline the left ventricle chamber. It makes pulmonary embolism (PE) very likely. Second: what does the ultrasound tell us about the condition? He was unresponsive to painful stimuli.
The morphology of V2-V4 is very specific in my experience for acute right heart strain (which has many potential etiologies, but none more common and important in EM than acute pulmonary embolism). CT angiogram showed extensive saddle pulmonary embolism. Now another, with ultrasound. On epinephrine and norepinephrine drips."
The Queen of Hearts read this ECG as OMI – Low Confidence Click here to sign up for QoH Access The providers taking care of this patient were concerned regarding his clinical history and initial ECG, so they next performed a bedside cardiac ultrasound. Speckle Tracking Echocardiography may provide another useful adjunct.
A bedside ultrasound should be done to assess volume and other etiologies of tachycardia, but if no cause of type 2 MI is found, the cath lab should be activated NOW. Then, part of the thrombus embolized into the LCx causing an inferoposterolateral OMI. (As Smith comment: this is diagnostic of OMI until proven otherwise.
A bedside cardiac ultrasound was normal, with no effusion. Clinically — despite an initial 2-fold increased troponin, the normal bedside Echo was reassuring against OMI or pulmonary embolism. He had the following EKG recorded: Low voltage, suggests effusion. see Ken's discussion of low voltage below) There is a QS-wave in V2.
Women and black patients were less frequently treated with minimally invasive therapy compared to men or non-Black patients, according to new data from the REAL-PE analysis which investigated catheter-based pulmonary embolism (PE) treatment. Late-breaking results from the study, for which Sahil A. PE affects around 900,000 people in the U.S.
CT angiogram chest: no aortic dissection or pulmonary embolism. Beware a negative Bedside ultrasound. He spent several days in the PICU, undergoing workup including: Serial troponins: rising from 5,700 ng/L (unknown if I or T) to greater than 25,000 ng/L (greater than the lab's upper limit of reporting). Pericarditis?
The post Ep 203 Intermediate Risk Pulmonary Embolism Risk Stratification, Management and Algorithm appeared first on Emergency Medicine Cases. Bourke Tillman and Anton as they explore the key decision points, pitfalls, and lifesaving strategies for managing intermediate-risk PE in the ED.
Check : [vitals, SOB, Chest Pain, Ultrasound] If the patient has Abdominal Pain, Chest Pain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Serious outcomes included death, arrhythmia, myocardial infarction, structural heart disease, pulmonary embolism, and hemorrhage.
The patient was found to have an embolic source. Provocative testing is very helpful for this Coronary Thrombus with lysis (one must do optical coherence tomography or at least intravascular ultrasound to find thes non-obstructive plaques that ruptured. Embolism with lysis. Need to find an embolic source.
Case continued A bedside cardiac ultrasound revealed grossly preserved left ventricular function, no appreciable wall motion abnormality, pericardial effusion, or obvious valvular abnormality.
On arrival in the ED, a bedside ultrasound showed poor LV function (as predicted by the Queen of Hearts) with diffuse B-lines. LAD: type III-IV vessel with a proximal thrombotic or embolic occlusion (TIMI 0 flow). I don't know what the device algorithm interpretation stated. Initial BP was 120/96, HR 102, SpO2 98%. Angiogram: 2.
Smith : This is classic for pulmonary embolism (PE). Acute pulmonary embolism was confirmed on CT angiogram: The patient did well. See our other acute right heart strain / pulmonary embolism cases: A man in his 50s with shortness of breath Another deadly triage ECG missed, and the waiting patient leaves before being seen.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content