This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
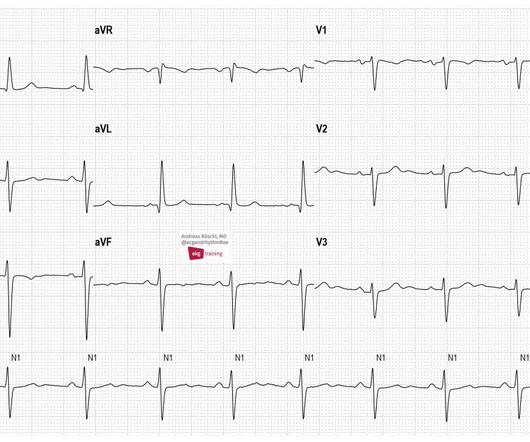
These are typical ECG changes that may indicate a pulmonary embolism. The patient has an acute pulmonary embolism. Sinus tachycardia may be present in acute pulmonary embolism. We see a sinus rhythm with left anterior fascicular block (LAFB) and conspicuous T-wave inversions in the inferior leads and in V1-V6.
male with pertinent past medical history including Atrial fibrillation, atrial flutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Description : Regular Wide Complex Tachycardia at a rate of about 160. SVT with aberrancy?
These are typical ECG changes that may indicate a pulmonary embolism. The patient has an acute pulmonary embolism. Sinus tachycardia may be present in acute pulmonary embolism. Wee see a SR with LAFB and conspicuous T-wave inversions in the inferior leads and in V1-V6. ECG 2 was taken from the same patient 1 year earlier.
He was started on a heparin drip and CTA of the chest was ordered to rule out pulmonary embolism. This is a case like many others posted (see list below) and the EKG from the patient’s original presentation can be quickly recognized as diagnostic for pulmonary embolism. In fact, Kosuge et al. Accessed May 28, 2024. This is a quiz.
CT of the chest showed no pulmonary embolism but bibasilar infiltrates. Even with tachycardia and a paced QRS duration of ~0.16 (And of course Ken's comments at the bottom) An elderly obese woman with cardiomyopathy, Left bundle branch block, and chronic hypercapnea presented hypoxic with altered mental status. She was intubated.
Introduction Multiple abnormal electrocardiographic findings have been documented in patients experiencing acute pulmonary embolism. Although sinus tachycardia is the most commonly encountered rhythmic disturbance, subsequent reports have highlighted other findings.
It shows sinus tachycardia with right bundle branch block. Taking a step back , remember that sinus tachycardia is less commonly seen in OMI (except in cases of impending cardiogenic shock). In patients with narrow QRS ( not this patient), this pattern is highly suggestive of acute pulmonary embolism. Both were wrong.
Here is his ECG: Original image, suboptimal quality Quality improved with PM Cardio digitization The ECG is highly suggestive of acute right heart strain, with sinus tachycardia, S1Q3T3, and T wave inversions in anterior and inferior with morphology consistent with acute right heart strain. Moreover, there is tachycardia.
Smith interpretation: This is highly likely to be due to extreme right heart strain and is nearly diagnostic of pulmonary embolism. It is of course pulmonary embolism. KEY Findings in ECG #1 include the following: Sinus tachycardia at ~110/minute. Junctional tachycardia? ).
Ken (below) is appropriately worried about pulmonary embolism from the ECG. A Closer LOOK at the ECG in Figure-1: The ECG in Figure-1 shows sinus tachycardia — with QRS widening due to complete RBBB. It is of an elderly woman who complained of shortness of breath and had a recent stent placed. What do you think?
An increase in myocardial oxygen demand due to tachycardia, elevated ventricular afterload (BP or Aortic stenosis), increased wall stretch, or a decrease in oxygen supply due to hypotension, anemia, hypoxia, sepsis, or a combination of all of the above. This latter part has been implicated in embolic CVA. Type II ischemia.
Smith comment: before reading anything else, this case screamed pulmonary embolism to me. CT chest showed left sided pulmonary embolism and a pulmonary infarct that had previously been mistaken for pneumonia. Instead, he was diagnosed with pneumonia — that turned out to be a left-sided pulmonary embolism that was initially missed.
The ECG is rather classic for pulmonary embolism, and indeed this was a large acute PE. This one is far more specific, as it is combined with sinus tachycardia and some T-wave inversion in V1-V3. and tachycardia, 1.8. this is highly suggestive of pulmonary embolism. This is a classic S1Q3T3. Most S1Q3T3 is not due to PE.
The morphology of V2-V4 is very specific in my experience for acute right heart strain (which has many potential etiologies, but none more common and important in EM than acute pulmonary embolism). CT angiogram showed extensive saddle pulmonary embolism. He had multiple cardiac arrests with ROSC regained each time. This is a quiz.
Genetic testing for hypertrophic cardiomyopathyassociated genes was performed in 72 patients.ResultsAmong the patients, 60 were classified as pureapical form, and 51 were classified as distaldominant form.
Notice I did not say "pulmonary embolism," because any form of severe acute right heart strain may produce this ECG. Differences of Pulmonary Embolism T-waves from Wellens' T-waves: 1. Acute coronary occlusion (especially during reperfusion) is very rarely accompanied by tachycardia. What is the answer?
This usually represents posterior OMI, but in tachycardia and especially after cardiac arrest, this could simply be demand ischemia, residual subendocardial ischemia due to the low flow state of the cardiac arrest. This prompted cath lab activation. On arrival to the ED, this ECG was recorded: What do you think?
Whenever you see tachycardia with bundle branch block, you should suspect that it is rate related BBB. First, as I have pointed out in posts on pulmonary embolism (see links), T-wave inversion of anterior infarction (Wellens' syndrome) almost always has an upright T-wave in lead III. Moreover, and importantly, there was sinus tach.
Tachycardia (or nearly) 2. And some similar ECGs from Pulmonary Embolism: A young woman with altered mental status and hypotension An elderly woman transferred to you for chest pain, shortness of breath, and positive troponin - does she need the cath lab now? Tachycardia, = 1.8. Poor R-wave progression 4. Kosuge et al.
The bedside echo showed a large RV (Does this mean there is a pulmonary embolism as the etiology?) When you suspect pulmonary embolism due to large RV on POCUS, always look for right axis deviation and a large R-wave in V1 because the large RV may be entirely due to chronic RVH, not acute PE. Here is his triage ECG: What do you think?
We can see enough to make out that the rhythm is sinus tachycardia. Tachycardia is unusual for OMI, unless the patient is in cardiogenic shock (or getting close). A bedside ultrasound should be done to assess volume and other etiologies of tachycardia, but if no cause of type 2 MI is found, the cath lab should be activated NOW.
They include myocardial ischemia, acute pericarditis, pulmonary embolism, external compression due to mass over the right ventricular outflow tract region, and metabolic disorders like hyper or hypokalemia and hypercalcemia. These are the conditions which have to be considered or excluded as they can sometimes manifest Brugada pattern on ECG.
The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis. The patient had been on a long drive, suggesting possible pulmonary embolism (this was unlikely given absence of tachyardia, hypoxia, or any other feature of PE), so we sent a d dimer.
If there are T-wave inversions and elevated trops in the context of persistent pain, think of other pathologies such as pulmonary embolism. That said, against acute PE — is the inconstancy of this patient's symptoms — the lack of tachycardia — and the lack of any other ECG signs of acute RV strain.
Clinically — despite an initial 2-fold increased troponin, the normal bedside Echo was reassuring against OMI or pulmonary embolism. This sinus tachycardia ( at ~130/minute ) — is consistent with the patient’s worsening clinical condition, with development of cardiogenic shock.
Patients with pulmonary embolism or aortic dissection who have normal variant ST elevation are at high risk of being diagnosed with pericarditis when what they have is far more serious!! The vast majority of cases with chest pain diffuse ST Elevation are due to Normal Variant ST Elevation, NOT to pericarditis.
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. Serious outcomes included death, arrhythmia, myocardial infarction, structural heart disease, pulmonary embolism, and hemorrhage.
Smith : This is classic for pulmonary embolism (PE). Acute pulmonary embolism was confirmed on CT angiogram: The patient did well. See our other acute right heart strain / pulmonary embolism cases: A man in his 50s with shortness of breath Another deadly triage ECG missed, and the waiting patient leaves before being seen.
Third, a slow motion segment showing delayed, brisk filling of the PDA due to dislodgment of a thrombus from contrast injection and distal embolization. A distal RCA lesion ( blue arrow ), Delayed brisk filling of an initially occluded PDA due to a thrombus dislodged during injection which embolized distally.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content