This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The Neuroguard Integrated Embolic Protection (IEP) system is an experimental treatment for carotid artery stenosis, also known as carotid artery disease, a condition in which fatty-waxy deposits known as plaque builds up and blocks the normal flow of blood in the large arteries on either side of the neck. Designed by Raleigh, N.C.-based
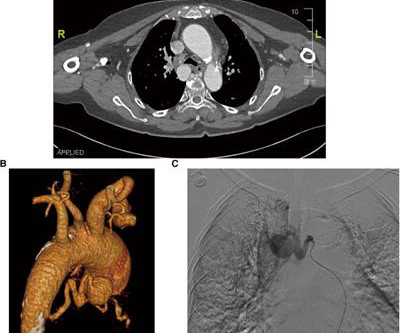
However, conventional surgical and transcatheter arterial embolization treatments are less effective. In the present case, a 76-year-old hypertensive woman was admitted with dizziness and diagnosed with an unruptured bronchial artery aneurysm, which was treated by transcatheter arterial embolization and aortic stent-graft.
Some of the late-breaking topics that will be covered include transcatheter aortic valve replacement (TAVR), peripheral artery disease (PAD), and pulmonary embolism (PE): Impact of Age on Procedural Timing for Asymptomatic Severe Aortic Stenosis: Results from the Early TAVR Trial The PERFORMANCE II Trial: A Prospective Multicenter Single Arm Investigation (..)
After preoperative evaluation, coil embolization was successfully performed to treat the pseudoaneurysm, resulting in a satisfactory outcome at the 1-year follow-up.ConclusionCoil embolization serves as an effective treatment option for ascending aortic pseudoaneurysm in BD when open surgical repair and stent graft placement are unsuitable.
In this phenomenon, a thrombus forms within the lumen of the stent graft component of the frozen elephant trunk prosthesis and puts the patient at risk for downstream embolization with visceral or lower limb ischemia. Therefore, the presence of ILT is associated with increased short-term mortality and morbidity.
IntroductionThe use of detachable coils for endovascular embolization of cerebral aneurysms has become a safe and effective alternative to direct surgical clipping in patients with ruptured aneurysmal subarachnoid hemorrhage. The post‐procedural complication rate proved to be higher than in non‐ruptured stent‐assisted coiling.
We describe a case of external carotid stenting with carotid stump coil occlusion.MethodsWe present a case report. Magnetic resonance imaging revealed embolic appearing strokes in the right middle cerebral artery territory (Figure 1A). The patient was treated with aspirin and ticagrelor for 3 months.
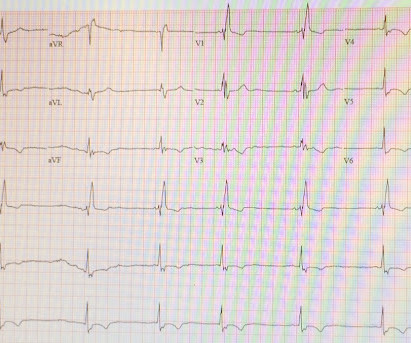
It is of an elderly woman who complained of shortness of breath and had a recent stent placed. Ken (below) is appropriately worried about pulmonary embolism from the ECG. Also, we know the patient had a stent. A few days before that, she had had an LAD stent for LAD occlusion. What do you think?
Registry data on nearly 10,000 patients in Japan show a high utilization of embolic protection devices and procedural safety in both symptomatic and asymptomatic patients.
Of note, patient had a with left cavernous‐ICA stent placement a month before the presentation and was noncompliant to antiplatelets. More people are getting flow divertors over the years and rate of flow diverter of ICA occlusion is 0.05%‐0.08% (2). In the emergency department (ED), her NIHSS was 28. ED presentation was 2.5
3 The third‐generation iteration of the Pipeline Embolization Device (PED) incorporates Shield technology, a phosphorylcholine coating designed to reduce thrombogenicity via mimicry of native cell membranes.4 IntroductionIndications for flow diversion for the treatment of cerebral aneurysms have increased remarkably in recent years.1
Purpose:Since the balloon protection device became unavailable in Japan three years ago, the DWI-positive rate after carotid artery stenting (CAS) has increased. We have developed a Proximal balloon Occlusion With forcEd aspiRation (POWER) technique to prevent distal embolization in CAS with the filter protection device.
With the advancement of endovascular coil devices, aneurysm embolization with coiling is becoming the more preferred treatment approach compared to craniotomy with microsurgical clipping. Primary outcomes were functional status recorded as modified Rankin scores (mRS) and radiographic occlusion rates documented as Raymond‐Roy scores.
The purpose of this study was to compare the outcomes of EVT for ICAD with those of cardiogenic cerebral embolism (CE) based on real-world data from a multicenter, prospective registry study (K-NET registry) involving 40 centers in Japan.Methods:The K-NET study enrolled 3187 EVTs in 2018-2021, of which 358 (11%) were ICAD and 1870 (59%) were CE.
BackgroundThe VenaTech Convertible Vena Cava Filter (VTCF) is a device designed for insertion into the inferior vena cava (IVC) to prevent life-threatening pulmonary embolism (PE).
Nature Reviews Cardiology, Published online: 02 April 2024; doi:10.1038/s41569-024-01020-2 In ST-segment elevation myocardial infarction, the role of interventional modification of thrombi in the coronary arteries before stenting is controversial.
IntroductionFlow diverters (FD) are stent‐type devices that enable the exclusion of intracranial aneurysms in clinical scenarios where coil‐type devices exhibit high failure rates. Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023.
She elected to undergo right MEV coil embolization. For management she underwent coil embolization of the right occipital vein, as this was the vessel the posterior auricular vein was draining into. Initially, he underwent stent‐assisted coiling of a high‐riding jugular bulb with no change in symptoms.
Coil embolization was performed for fifty‐four patients using various adjunctive techniques (simple, 7; double catheter, 15; balloon neck remodeling, 7; stent‐assisted, 26 (LVIS Jr., The surgical results revealed complete coil embolization in 27, neck remnant in 26, and dome filling in 1 patient(s). 12; ATLAS, 14).
This catheter is designed to help deliver interventional devices into the blood vessels in the brain, allowing doctors to place devices like stents or coils, to treat neurovascular diseases and conditions. This type of catheter is commonly used in procedures where precise navigation and access to blood vessels in the brain are required.
Baseline characteristics and technical and clinical outcomes were compared between the two groups, with subgroup analysis in first-line thrombectomy techniques, including ADAPT, stent retriever, and Solumbra. In terms of clinical outcomes, the BGC group had a lower rate of distal embolization (overall: 8.8%
The stent–aspiration (Solumbra) technique uses a large bore aspiration catheter with a stent retriever device for potential synergistic effects. The technique involves deploying a stent retriever through microcatheter and large bore aspiration catheter like ACE 68 (Penumbra, Inc.),
Ischaemic events were defined as myocardial infarction, stroke, transient ischaemic attack or peripheral embolism at 1 year. Patterns of Non-adherence to Anti-Platelet Regimen in Stented Patients (PARIS) and Coronary Revascularisation Demonstrating Outcome Study in Kyoto (CREDO-Kyoto) integer scoring systems were tested.
Hemodynamic and embolic factors attribute towards the microembolization from the proximal carotid stump through the external carotid artery (ECA), into the facial artery and IMax and their distal branches which anastomose with the ophthalmic artery, causing the emboli to end up in the major branches of the carotid terminus.
This was treated with a drug-eluting stent, but TIMI 3 flow was not achieved. Due to ongoing shock despite initial mechanical support, the patient was escalated to an Impella CP device after a transthoracic echo confirmed no left ventricle thrombus. Once stabilized, intravascular ultrasound showed significant thrombus and plaque in the LAD.
We studied the effects of COA treatment with FD alone or in combination with coil embolization, based on the origin of the ophthalmic artery in‐relation to the aneurysm sac.MethodsRetrospective analysis of a prospectively collected tertiary center database. directly from the aneurysm fundus, B. aneurysm neck, C. Median age was 55.
Statistical analysis was performed to identify predictors of inadequate occlusion.ResultsA total of 51 patients underwent endovascular embolization using the WEB device with a mean follow‐up of 14.9 Thromboembolic complications and retreatments were recorded. Most of the patients (92.1%) were functionally independent at presentation.
He took another look and realized that the culprit was indeed in the proximal RCA and that the thrombus had embolized distally. And so he put the stent in the proximal RCA. I asked if he was sure about this, because the ECG would indicate a proximal RCA occlusion with RV MI.
However, IVT's efficacy on stent retriever (SR) and aspiration thrombectomy (ASP) outcomes specifically remain unclear. Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. IntroductionEfficacy and safety of intravenous thrombolysis (IVT) in patients undergoing mechanical thrombectomy (MT) is still debatable.
A subanalysis of the TIGER study data was performed in order to assess the effectiveness and safety of Tigertriever in small and large clot sizes.Methods:The TIGER study was a single arm, prospective, multi-center trial assessing the efficacy and safety of the Tigertriever, a radially-adjustable stent retriever, for LVO-related stroke.
IntroductionThe 2015 American Heart Association Guidelines recommended mechanical thrombectomy with stent‐retriever devices. Compared with 2012‐2014, the 2015‐2019 cohort showed increased odds of ICH and shock while the odds of DVT, pulmonary embolism, pneumonia, and UTI were significantly lower.
Coil embolization (CE) is safer and more efficacious in the treatment of BTAs compared to open surgery but has increased rate of recanalization. Stents approved by FDA after 2014 (used in 13 cases) had a greater rate of retreatment (46.2% We also found an association with time of approval to retreatment. vs. 10.7%).
On day 3 of hospitalization she underwent coronary angiography, revealing a 95% lesion in the mid-LAD which was stented. A new right bundle branch block in a sick patient with chest pain and/or shortness of breath is a worrisome finding concerning for LAD occlusion or significant pulmonary embolism.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction.
It was opened and stented. LV aneurysm puts them at risk for a mural thrombus, which puts them at risk for embolism, especially embolic stroke. One can now see that these large R-waves are Q-waves and the ST depression, as seen from the posterior wall, is really ST elevation! The cath lab was activated.
Several hours later, angiogram showed: Culprit lesion mid LAD, 75% stenosis, TIMI 3, thrombotic, likely the source of the distal LAD 100% embolic occlusion, with TIMI 0 flow. The culprit mid LAD lesion was stented. It is not clear in the report whether thrombectomy was performed on the distal LAD occlusion.
IntroductionMechanical thrombectomy using stent retrievers and aspiration techniques has emerged as the standard of care for patients with acute ischemic stroke (AIS) secondary to emergent large vessel occlusion (LVO). Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023.
And they of course activated the cath lab immediately, where he was found to have acute thrombotic occlusion (TIMI 0) of the proximal LAD, as well as embolic D1 occlusion. LAD and D1 were stented, but flow unfortunately could not be well restored despite efforts (they list the post intervention TIMI flow still as 0).
The patient had been on a long drive, suggesting possible pulmonary embolism (this was unlikely given absence of tachyardia, hypoxia, or any other feature of PE), so we sent a d dimer. [We It was opened and stented with a door to balloon time of about 120 minutes (this is long for STEMI, but very short for a high risk Non STEMI).
You may see a filling defect in distal LAD, most probably due to an embolization from proximal lesion. The lesion was successfully stented, but it was unfortunately done after a significant myocardial loss. Also note that LAD does not extensively wrap-around apex and supply inferior wall. Aslanger as one of the co-authors ).
INTERVENTION * Successful angioplasty and stenting (drug eluting) of the mid LAD * Successful angioplasty of the ostial 1st diagonal Learning points: 1. If there are T-wave inversions and elevated trops in the context of persistent pain, think of other pathologies such as pulmonary embolism. Young women do get acute MI 2.
Bi-phasic scan showed no dissection or pulmonary embolism. The lesion was successfully stented. --In summary, some subtle findings which do not fit into a pattern, therefore may be nonspecific ECG changes which are encountered everyday. Aspirated thrombotic material. Here is the post-intervention angiogram and post-PCI ECG.
However, by the time of the angiogram it had embolized distally, and had only done so after the right sided ECG was recorded. He did, found the true culprit, and went back in to stent it. See this case in which I saw STE in V1 and called the angiographer to suggest he look more closely at the angiogram.
It was treated with and dual "kissing balloons" and drug eluting stents. Here is the post stent ECG: There is greater than 50% resolution of ST elevation (all but diagnostic of successful reperfusion) and Terminal T-wave inversion (also highly suggestive of successful reperfusion). TIMI flow is 0. Door to balloon time was 51 minutes.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content