This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Some of the late-breaking topics that will be covered include transcatheter aortic valve replacement (TAVR), peripheral artery disease (PAD), and pulmonary embolism (PE): Impact of Age on Procedural Timing for Asymptomatic Severe Aortic Stenosis: Results from the Early TAVR Trial The PERFORMANCE II Trial: A Prospective Multicenter Single Arm Investigation (..)
The LM has an irregular 30% distal stenosis, followed by an 80% ostial LAD stenosis, and total occlusion of the LAD proximally with TIMI grade 1 flow in the distal vessel. The LCX demonstrates an ostial 80% stenosis prior to the bifurcation of a large OM artery. This latter part has been implicated in embolic CVA.
The objective of this report was to enhance clinicians' awareness of embolism susceptibility. It is recommended that young and middle-aged patients with severe coronary artery stenosis undergo screening for embolism.
The risk of stroke recurrence among patients with ICAD-related stroke is the highest among those with confirmed stroke and stenosis ≥70%. In fact, the 1-year recurrent stroke rate of >20% among those with stenosis >70% is one of the highest rates among common causes of stroke.
The Woven EndoBridge (WEB) is an ellipsoid embolization device designed to provide intrasaccular flow disruption along the aneurysm neck, which has been proven to be an effective method in treating a wide spectrum of wide‐necked bifurcation aneurysms. Multifocal severe stenosis was noted in the right distal right M1 and right M2 divisions.
Introduction:A new Plaque-RADS classification (I-IV) is proposed to categorize the degree of carotid plaque instability and risk of embolic ischemic stroke.
The goal of the PROTECTED TAVR trial was to evaluate the efficacy of intraprocedural cerebral embolic protection (CEP) in reducing strokes among patients undergoing transfemoral TAVR for aortic stenosis.
Recent literature identifies venous etiologies as the most common cause of pulsatile tinnitus, including venous sinus stenosis, venous diverticula, and the less common enlarged mastoid emissary vein (MEV). Emissary veins are residual connections between the extracranial venous system of the head and the intracranial venous system.
Known complications associated with cryoablation include tamponade, phrenic nerve injury, stroke, pulmonary embolism, pulmonary vein stenosis, and atrioesophageal fistulas. Cryoablation for atrial fibrillation is a widely used technique for pulmonary vein isolation.
Background:High-risk non-stenosing carotid plaque features are emerging as a possible source of embolism in the setting of ESUS. It is essential to conduct algorithms, scoring systems and prediction models to determine which plaque features are highly associated with embolism.
She elected to undergo right MEV coil embolization. For management she underwent coil embolization of the right occipital vein, as this was the vessel the posterior auricular vein was draining into. Catheter venography showed an enlarged right posterior condylar vein (PCV) and right IJ stenosis. mm in its widest dimension).
Previous studies have noted that ICAD-related LVOs, compared to embolic occlusions, have longer procedural times and lower successful reperfusion rates. ICAD group was defined as persistent occlusion or residual stenosis at the initial occlusion site. However, clinical outcomes remain similar.
Coil embolization was performed for fifty‐four patients using various adjunctive techniques (simple, 7; double catheter, 15; balloon neck remodeling, 7; stent‐assisted, 26 (LVIS Jr., The surgical results revealed complete coil embolization in 27, neck remnant in 26, and dome filling in 1 patient(s). 12; ATLAS, 14).
Stenosis of the external carotid artery in such patients can be a source of atheroembolism or hypoperfusion. Magnetic resonance imaging revealed embolic appearing strokes in the right middle cerebral artery territory (Figure 1A). The patient was treated with aspirin and ticagrelor for 3 months.
Even in patients whose moderate stenosis undergoes thrombosis, most angiograms show greater than 50% stenosis after the event. However, one can certainly imagine that many thromboses of non-obstructive lesions completely lyse and do not leave a stenosis on same day or next day angiogram.
We have developed a Proximal balloon Occlusion With forcEd aspiRation (POWER) technique to prevent distal embolization in CAS with the filter protection device. Symptomatic stenosis (63.9% The concept of this technique was to standardize the three points: (1) aspiration force, (2) timing of aspiration and (3) use of balloon guiding.
On follow up angiography, there was a large OM1 and small AV groove Cx/LPL visible as the vessel re-canalized LAD is noted to have diffuse 50% stenosis in the proximal segment and is occluded immediately beyond a small D1 RCA is a medium-large caliber vessel and supplies a medium rPDA, medium rPLA1, and three small rPLA branches. TIMI-0 flow.
Background and purpose:The aortic complicated lesion (ACL) is a notable embolic source of cryptogenic stroke (CS) observed in 10-60 % of patients. Stroke, Volume 55, Issue Suppl_1 , Page ATP257-ATP257, February 1, 2024. Although the antithrombotic and statin therapy are certainly effective, the recurrence of aortogenic stroke is not rare.
LAD plaque with 0-25 percent stenosis. The LAD has moderate 40% ostial-proximal LAD stenosis and severe 90% mid LAD stenosis involving first diagonal branch. --The If there are T-wave inversions and elevated trops in the context of persistent pain, think of other pathologies such as pulmonary embolism.
1-4 Surprisingly, serial angiographic studies have revealed that the plaque at the site of the culprit lesion of a future acute myocardial infarction often does not cause stenosis that, as seen on the antecedent angiogram, is sufficiently severe to limit flow. There may be a chronic tight stenosis and a non-obstructed lesion that thrombosed.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
So it will not produce a true LV to aorta pullback tracing, which is required in cases like aortic stenosis. It is used for pulmonary angiography by the transfemoral route and it is also used for clot lysis in pulmonary embolism. When the tip is in the left ventricle, this region will be in the aorta sometimes.
Low LV filling pressures are due to several etiologies, most commonly due to volume depletion (dehydration or hemorrhage), but also due to other etiologies including, but not limited to: mitral stenosis, pulmonary hypertension (chronic, or due to pulmonary embolism), or poor RV performance.
The interventional cardiologist was not initially convinced this was ACS and recommended CT pulmonary angiography to rule out pulmonary embolism. CT Aortogram revealed: No pulmonary embolism, No aortic dissection. The pain returned/worsened , and the patient was then started on a nitroglycerin drip.
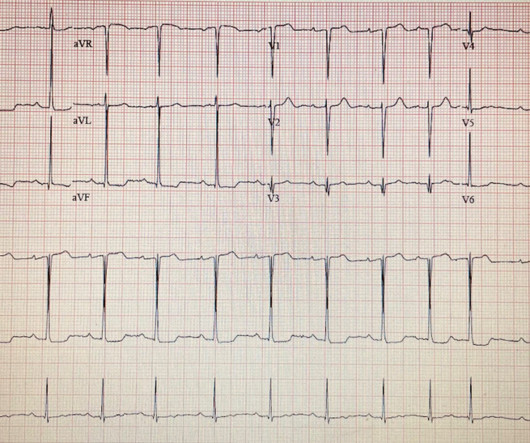
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. This is written by Willy Frick, an amazing cardiology fellow in St. He described it as "10/10" intensity, radiating across his chest from right to left.
pulmonary embolism, sepsis, etc.), distal stenosis or occluded small branches), and 3) nonischemic causes for myocyte injury (e.g., Coronary thrombosis or embolism can result in MINOCA, either with or without a hypercoagulable state. The diagnosis of MINOCA should exclude: 1) other overt causes for elevated troponin (e.g.,
The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis. The patient had been on a long drive, suggesting possible pulmonary embolism (this was unlikely given absence of tachyardia, hypoxia, or any other feature of PE), so we sent a d dimer. [We
CT pulmonary angiogram was negative for pulmonary embolism. Cath was done at around 9AM: Culprit lesion mid-LAD, 99% stenosis, pre-intervention TIMI flow not listed, PCI performed with TIMI 3 flow and 0% stenosis resulting. Normal RV, no significant valvular stenosis or regurgitation. Chest x-ray was read as normal.
They found non-obstructive CAD, with only a 20% stenosis of OM2 and 10% RCA. Patients with pulmonary embolism or aortic dissection who have normal variant ST elevation are at high risk of being diagnosed with pericarditis when what they have is far more serious!! No acute culprit. He was admitted to cardiology.
About a fifth of all ischemic strokes are attributed to embolization of ruptured atherosclerotic plaque from carotid arterial stenosis. But it has been difficult to predict which person with asymptomatic carotid artery stenosis is likely to progress to symptomatic carotid disease and stroke. J Am Coll Cardiol. 2024.03.389.
BACKGROUND:A modified computed tomography angiography (CTA)based Carotid Plaque Reporting and Data System (Plaque-RADS) classification was applied to a cohort of patients with embolic stroke of undetermined source to test whether high-risk Plaque-RADS subtypes are more prevalent on the ipsilateral side of stroke.
The Neuroguard Integrated Embolic Protection (IEP) system is an experimental treatment for carotid artery stenosis, also known as carotid artery disease, a condition in which fatty-waxy deposits known as plaque builds up and blocks the normal flow of blood in the large arteries on either side of the neck.
Several hours later, angiogram showed: Culprit lesion mid LAD, 75% stenosis, TIMI 3, thrombotic, likely the source of the distal LAD 100% embolic occlusion, with TIMI 0 flow. The culprit mid LAD lesion was stented. It is not clear in the report whether thrombectomy was performed on the distal LAD occlusion.
In addition, the top left blue arrow indicates a section in the LAD with a severe stenosis, likely the culprit for the prior L A D occlusion which has since recanalized. Then, part of the thrombus embolized into the LCx causing an inferoposterolateral OMI. (As There are also diagonal branches which are not well visualized.
Kown, Asan Medical Center, Seoul, Korea Golden Bridge II Effect of an Artificial Intelligence-Based Clinical Decision Support System on Stroke Care Quality and Outcomes in Patients With Acute Ischemic Stroke : A Cluster-Randomized Clinical Trial: Zixiao Li, Beijing Tiantan Hospital, Capital Medical University, Beijing, China Friday, Feb.
The patient was found to have an embolic source. Embolism with lysis. Need to find an embolic source. Here it is annotated in red: Our extremely smart radiologist, Gopal Punjabi , assures me that this finding can only be due to myocardial infarction, not myocarditis. So this is "MINOCA". As I wrote in that Nov.
The TAVR UNLOAD trial also found that there’s not much to gain by performing earlier TAVR in patients with HFrEF and moderate aortic stenosis. The PROTECTED TAVR trial rounded out the major TAVR late-breakers, finding that cerebral embolic protection’s benefits varied geographically, and somehow didn’t reduce overall strokes.
Background Current guidelines recommend transcatheter aortic valve implantation (TAVI) for patients with aortic stenosis and porcelain aorta (PA). These findings might influence cerebral embolic protection device use in patients with PA.
Angiogram: Severe two-vessel coronary artery disease of a left dominant system including 70 to 80% stenosis involving the distal left main/bifurcation. By itself seeing this ECG pattern does not necessarily mean that the patient has a pulmonary embolism. The estimated left ventricular ejection fraction is 64%.
No pulmonary embolism is identified. First obtuse marginal also had an 80% stenosis and was stented. While in the ED, patient's pain worsened to previous severity of 6/10 pain and improved to 3/10 on NTG drip. CT Angio Chest IMPRESSION 1. No thoracic aortic hematoma, aneurysm or dissection.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content