This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BACKGROUND:Prior clinical trials have demonstrated the efficacy of ultrasound-facilitated catheter-directed thrombolysis (USCDT) for the treatment of acute intermediate-risk pulmonaryembolism (PE) using reduced thrombolytic doses and shorter infusion durations. Circulation: Cardiovascular Interventions, Ahead of Print.
The risk factors for postoperative embolism included Black race, interstitial fibrosis, advanced-stage disease requiring bilobectomy or pneumonectomy, and increased operative duration. occurrence of postoperative PE in patients undergoing a first-time pulmonary resection for lung cancer. occurrence of postoperative VTE and a 1.3%
He was started on a heparin drip and CTA of the chest was ordered to rule out pulmonaryembolism. This is a case like many others posted (see list below) and the EKG from the patient’s original presentation can be quickly recognized as diagnostic for pulmonaryembolism. Now another, with ultrasound. This is a quiz.
This Best Case Ever elucidates the practical challenges of working up pregnant patients in the ED with a suspicion of pulmonaryembolism. Since this recording, the first ever multi-center prospective outcome study looking at the pulmonaryembolism workup in pregnancy was published in the Annals of Internal Medicine.
Notably, acute massive pulmonaryembolism (PE) with bilateral atrial thrombosis is an exceptional occurrence in CAPS. Acute pulmonaryembolism (PE) is a common cardiovascular disease that progresses rapidly and has a high mortality rate. It primarily affects small vessels, seldom impacting large vessels.
Genetic protein S (PS) deficiency caused by PROS1 gene mutation is an important risk factor for hereditary thrombophilia.Case introductionIn this case, we report a 28-year-old male patient who developed a severe pulmonaryembolism during his visit. Ultrasound showed no thrombosis in the veins of both lower limbs.
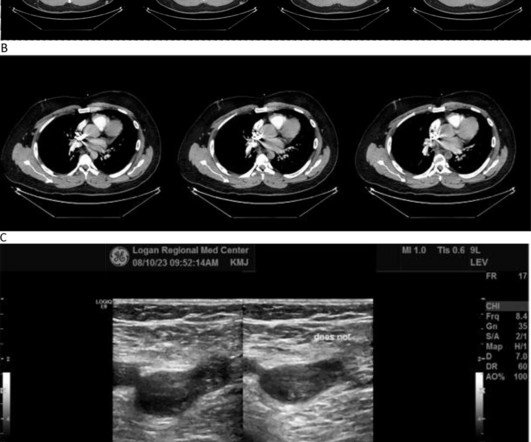
He was requiring supplemental oxygen and an initial bedside cardiac ultrasound was unremarkable. Despite his large clot burden, there was absence of obstructive shock.Transthoracic Echocardiogram and bilateral duplex venous ultrasound were obtained to evaluate for right heart strain and clot burden. Cardiology was consulted.
In patients with narrow QRS ( not this patient), this pattern is highly suggestive of acute pulmonaryembolism. Answer : Bedside ultrasound! Smith : RV infarct may also have this appearance on ultrasound. In PE, there is almost always some hypoxia without any pulmonary edema.
We have seen this pattern in many pts with acute right heart strain on this blog. __ Smith : The combination of T-wave inversion in V1-V3 and in lead III is very specific for acute pulmonaryembolism. Acute pulmonaryembolism was confirmed on CT: The patient did well with treatment. Now another, with ultrasound.
A venous Doppler ultrasound revealed an extensive right lower extremity DVT. Further imaging with a computed tomography (CT) pulmonaryembolism (PE) protocol scan of the chest and abdomen identified IVC agenesis along with pulmonary emboli in the left central pulmonary arteries.
Bedside cardiac ultrasound showed moderately decreased LV function. CT of the chest showed no pulmonaryembolism but bibasilar infiltrates. (And of course Ken's comments at the bottom) An elderly obese woman with cardiomyopathy, Left bundle branch block, and chronic hypercapnea presented hypoxic with altered mental status.
male with pertinent past medical history including Atrial fibrillation, atrial flutter, cardiomyopathy, PulmonaryEmbolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Bedside ultrasound showed volume depletion and no pulmonary edema.
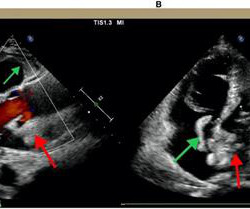
A bedside cardiac ultrasound was recorded: Here is a still image of the echo: The red arrows outline the right ventricle and the yellow arrows outline the left ventricle chamber. It makes pulmonaryembolism (PE) very likely. The small LV implies very low LV filling pressures, which implies low pulmonary venous pressure.
In this month's EM Quick Hits podcast, Anand Swaminathan on tips and tricks in polytrauma, Rohit Mohindra on diagnosis and management of toxic megacolon, Jesse McLaren on ECG in pulmonaryembolism, Victoria Myers on approach to the patch call for cardiac arrest, Brit Long on when to do a CT head before LP, Salim Rezaie on nebulized ketamine - the ketaBAN (..)
The morphology of V2-V4 is very specific in my experience for acute right heart strain (which has many potential etiologies, but none more common and important in EM than acute pulmonaryembolism). CT angiogram showed extensive saddle pulmonaryembolism. Now another, with ultrasound. What is the Diagnosis?
Smith comment: before reading anything else, this case screamed pulmonaryembolism to me. I would do bedside ultrasound to look at the RV, look for B lines as a cause of hypoxia (which would support OMI, and argue against PE), and if any doubt persists, a rapid CT pulmonary angiogram.
Ken (below) is appropriately worried about pulmonaryembolism from the ECG. What I had not told him before he made that judgement is that the patient also had ultrasound B-lines of pulmonary edema. I was told that the Queen of Hearts had called it OMI with high confidence. What do you think?
My opinion was that it was not a cath lab case, but I did suggest they do a bedside ultrasound to look for an anterior wall motion abnormality. The RV was small and IVC empty, making pulmonaryembolism extremely unlikely. The RV was small and IVC empty, making pulmonaryembolism extremely unlikely.
Rob always wished he had x-ray vision…but since he possesses no special powers…using Point-of-Care Ultrasound (POCUS) is the next closest thing. Robert Simard, an Emergency Physician at North York General Hospital and Sunnybrook Health Sciences Centre in Toronto.
Here is the cardiac ultrasound: The orange colored area is the Definity contrast in the chambers of the heart. This is known as McConnell's sign, and is described for PulmonaryEmbolism ; here we see it in right ventricular MI. The RV is on the left (circled below). Based on the appearance of the IVC, the RA pressure is low.
The ways to tell for certain include intravascular ultrasound (to look for extra-luminal plaque with rupture) or "optical coherence tomography," something I am entirely unfamiliar with. pulmonaryembolism, sepsis, etc.), Coronary thrombosis or embolism can result in MINOCA, either with or without a hypercoagulable state.
Women and black patients were less frequently treated with minimally invasive therapy compared to men or non-Black patients, according to new data from the REAL-PE analysis which investigated catheter-based pulmonaryembolism (PE) treatment. Late-breaking results from the study, for which Sahil A.
CT angiogram chest: no aortic dissection or pulmonaryembolism. Serial chest xrays: progressive bilateral pulmonary edema. Beware a negative Bedside ultrasound. No further troponins were measured. This gets drilled into them. Chest Pain in a Male in his 20's; Inferior ST elevation: Inferior lead "early repol" diagnosed.
Patients with pulmonaryembolism or aortic dissection who have normal variant ST elevation are at high risk of being diagnosed with pericarditis when what they have is far more serious!! Beware a negative Bedside ultrasound. You diagnose pericarditis at your peril! Acute MI is frequently misdiagnosed as pericarditis.
A bedside cardiac ultrasound was normal, with no effusion. and the patient was converted to veno-venous (V-V) ECMO due to persistent pulmonary insufficiency. Clinically — despite an initial 2-fold increased troponin, the normal bedside Echo was reassuring against OMI or pulmonaryembolism.
Check : [vitals, SOB, Chest Pain, Ultrasound] If the patient has Abdominal Pain, Chest Pain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Serious outcomes included death, arrhythmia, myocardial infarction, structural heart disease, pulmonaryembolism, and hemorrhage.
Smith : This is classic for pulmonaryembolism (PE). Acute pulmonaryembolism was confirmed on CT angiogram: The patient did well. Cardiac Ultrasound may be a surprisingly easy way to help make the diagnosis Answer: pulmonaryembolism. Now another, with ultrasound. What is the Diagnosis?
Case continued A bedside cardiac ultrasound revealed grossly preserved left ventricular function, no appreciable wall motion abnormality, pericardial effusion, or obvious valvular abnormality. Also: electrical instability, pulmonary edema, or hypotension. In this case, there was electrical instability (Mobitz II block).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content