This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Novartis initially prioritized its treatments for heart failure and plaque-clogged arteries when it spun-off abelacimab but continued to monitor the Factor XI race, leading to its choice to take the baton back from Anthos.
Introduction:A new Plaque-RADS classification (I-IV) is proposed to categorize the degree of carotid plaque instability and risk of embolic ischemic stroke. Carotid total plaque thickness and ulceration were scored by a neuroradiologist blinded to stroke side. N=188 plaques) met criteria.
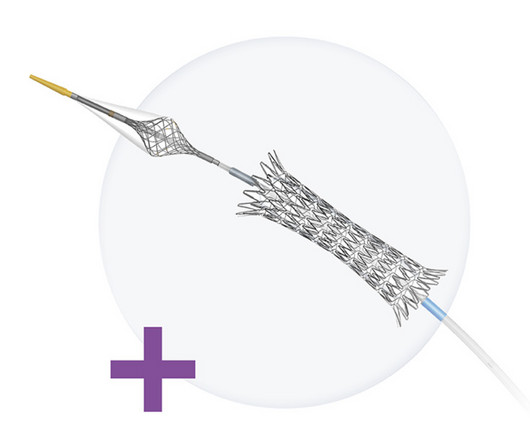
The Neuroguard Integrated Embolic Protection (IEP) system is an experimental treatment for carotid artery stenosis, also known as carotid artery disease, a condition in which fatty-waxy deposits known as plaque builds up and blocks the normal flow of blood in the large arteries on either side of the neck.
Background:High-risk non-stenosing carotid plaque features are emerging as a possible source of embolism in the setting of ESUS. We utilized Fisher’s exact test to compare the frequencies of reporting each plaque characteristic.Results:We analyzed 152 CTA reports in depth.
BACKGROUND:Aortic arch plaques are associated with an increased risk of ischemic stroke in patients with cryptogenic stroke or prior embolic events. Arch plaques were assessed by suprasternal transthoracic echocardiography; plaques ≥4 mm in thickness were classified as large plaques. Stroke, Ahead of Print.
BackgroundComplex aortic plaque (CAP) is a potential embolic source in patients with cryptogenic stroke (CS). Most studies (74%) used ≥4 mm plaque thickness as the imaging criterion for CAP although ≥1 mm (N=1, CTA), ≥5 mm (N=5, TEE), and ≥6 mm (N=2, CTA) were also reported. 0.41],I2=94%). I2=95%) for TEE; 0.23 (95% CI, 0.15–0.34;I2=87%)
BackgroundDisambiguation of embolus pathogenesis in embolic strokes is often a clinical challenge. One common source of embolic stroke is the carotid arteries, with emboli originating due to plaque buildup or perioperatively during revascularization procedures.
The mechanisms by which ICAD causes stroke include plaque rupture with in situ thrombosis and occlusion or artery-to-artery embolization, hemodynamic injury, and branch occlusive disease.
MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. See "Mechanisms of acute coronary syndromes related to atherosclerosis".)
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction.
Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates). This latter part has been implicated in embolic CVA. The underlying etiology is either Type 1 or Type II ischemia, although sometimes there’s overlap of both. Type I ischemia. Type II ischemia.
A pathological classification of no-reflow was proposed: structural no-reflow—microvessels within the necrotic myocardium exhibit loss of capillary integrity (it is usually irreversible)—and functional no reflow—patency of microvasculature is compromised due to distal embolization, spasm, ischemic injury, reperfusion injury.
Coronary Artery Disease (CAD) CAD, which involves the narrowing or blockage of coronary arteries due to plaque buildup, can reduce blood flow to the heart. Blood Clots: An enlarged heart is more prone to developing blood clots, which can lead to stroke or pulmonary embolism.
Integration with carotid plaque data and diffusion coefficient analysis revealed shared transcriptional programs existing in a continuum, progressing from asymptomatic plaque to embolized thrombus.
About a fifth of all ischemic strokes are attributed to embolization of ruptured atherosclerotic plaque from carotid arterial stenosis. But it has been difficult to predict which person with asymptomatic carotid artery stenosis is likely to progress to symptomatic carotid disease and stroke.
If the arrest was caused by acute MI due to plaque rupture, then the diagnosis is MINOCA. Here is my comment on MINOCA: "Non-obstructive coronary disease" does not necessarily imply "no plaque rupture with thrombus." They often cannot even be recognized as culprits, as fissured or ulcerated plaque. myocarditis).
As in all ischemia interpretations with OMI findings, the findings can be due to type 1 AMI (example: acute coronary plaque rupture and thrombosis) or type 2 AMI (with or without fixed CAD, with severe regional supply/demand mismatch essentially equaling zero blood flow). CT angiogram showed extensive saddle pulmonary embolism.
Once stabilized, intravascular ultrasound showed significant thrombus and plaque in the LAD. Due to ongoing shock despite initial mechanical support, the patient was escalated to an Impella CP device after a transthoracic echo confirmed no left ventricle thrombus. This was treated with a drug-eluting stent, but TIMI 3 flow was not achieved.
To prove there is no plaque rupture, you need to do intravascular ultrasound (IVUS). An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!! One of the most common is rupture of a non-obstructive plaque, with thrombus formation and OMI that spontaneously lyses and leaves a wide open artery. It can only be seen by IVUS.
We have developed a Proximal balloon Occlusion With forcEd aspiRation (POWER) technique to prevent distal embolization in CAS with the filter protection device. Purpose:Since the balloon protection device became unavailable in Japan three years ago, the DWI-positive rate after carotid artery stenting (CAS) has increased.
Background:Intracranial Atherosclerosis (ICAS) leads to stroke by perforator disease, artery to artery embolism, and impaired distal flow/perfusion. While medical treatment is likely to stabilize atherosclerotic plaques, it is unlikely to improve distal perfusion in the acute setting.
MRI at the time showed an acute embolic infarct in left MCA territory, and a CTA showed a sub‐occlusive thrombus vs. atherosclerotic plaque in the superior branch of the left MCA. His first stroke was preceded by about 1 week of intermittent confusion and right arm tingling.
ET Main Tent (Hall B1) Coronary Sinus Reducer for the Treatment of Refractory Angina: A Randomised, Placebo-controlled Trial (ORBITA-COSMIC) Transcatheter Aortic Valve Implantation Versus Surgical Aortic Valve Replacement in Patients at Low to Intermediate Risk: One Year Outcomes of the Randomized DEDICATE-DZHK6 Trial Effect of Alcohol-mediated Renal (..)
She had some very minor plaque but certainly nothing that could explain the heart attack and therefore she was discharged with a diagnosis of MINOCA i.e She agreed and we performed an angiogram and we were fully expecting a blockage but interestingly there weren’t any.
LAD plaque with 0-25 percent stenosis. If there are T-wave inversions and elevated trops in the context of persistent pain, think of other pathologies such as pulmonary embolism. Now, with elevated troponins, Wellens' syndrome is likely. A CT Coronary angiogram was ordered. CAD-RADS category 1. --No Possibility #2: As per Dr.
Today, they viewed the angiogram and concluded that the thrombus at the mid RCA must have extended proximally from the culprit ruptured plaque, extending proximal to the RV marginal branch and temporarily occluding it. However, by the time of the angiogram it had embolized distally, and had only done so after the right sided ECG was recorded.
CT angiogram chest: no aortic dissection or pulmonary embolism. Only after her troponin peaked at 500,000 ng/L did she get her angiogram, which showed a 100% left main occlusion due to ruptured plaque. No further troponins were measured. Serial chest xrays: progressive bilateral pulmonary edema. Diagnostic of Massive OMI.
Then, part of the thrombus embolized into the LCx causing an inferoposterolateral OMI. (As As an aside, the LCx OMI is a type 2 event, since it is due to supply-demand mismatch from thrombus, and not due to atherosclerotic plaque rupture or erosion). This resulted in anterior/apical infarct and apical thrombus formation.
BACKGROUND:A modified computed tomography angiography (CTA)based Carotid Plaque Reporting and Data System (Plaque-RADS) classification was applied to a cohort of patients with embolic stroke of undetermined source to test whether high-risk Plaque-RADS subtypes are more prevalent on the ipsilateral side of stroke.
BACKGROUND:Many ischemic strokes are diagnosed as embolic strokes of undetermined source (ESUS). Recent evidence suggests that nonstenotic carotid plaque (nsCP) may be a substantial contributor to the risk for ESUS. Stroke, Ahead of Print.
Angiogram: --"Suspected culprit for the patient's non-ST elevation myocardial infarction with refractory chest discomfort (although it had resolved prior to arrival to the cardiac catheterization lab), is a ruptured plaque in the distal circumflex with local embolic occlusion of the distal OM 3."
Third, a slow motion segment showing delayed, brisk filling of the PDA due to dislodgment of a thrombus from contrast injection and distal embolization. A distal RCA lesion ( blue arrow ), Delayed brisk filling of an initially occluded PDA due to a thrombus dislodged during injection which embolized distally. link] Bentzon, J.
And it is definitely possible that a more proximal LCx lesion ruptured and produced distal embolism. And in a study like COMPLETE or MULTISTARS AMI, you are stenting an acute plaque rupture (the culprit) and non-ruptured, non-culprit and hence essentially stable plaques. Some others worried about the RCA as a possible culprit.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content