This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
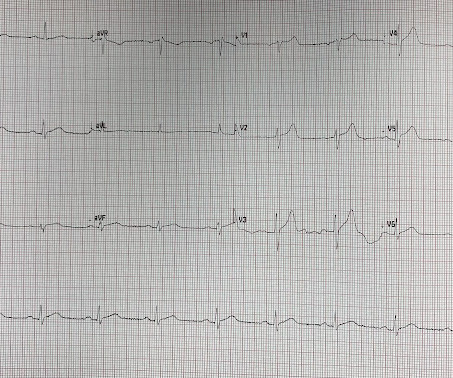
mm has been described in normal subjects) Overall impression: In my opinion and experience, this ECG most likely represents a normal baseline ECG, but with a small chance of pericarditis instead. I texted this to Dr. Smith without any information, and this was his reply: "This could be pericarditis but probably is normal variant."
But there was some doubt as to whether it might be pericarditis because of the ST elevation in I and II, without ST depression in III. Add that to "sharp" pain and a 33 year old, and it is easy to convince yourself that this is, indeed, pericarditis. This is a good sign for myocardial infarction and does not happen in pericarditis.
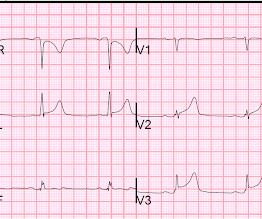
Here is his initial ED ECG: The R-wave in V4 extends to 33 mm, the computerized QTc is 372 ms The only available previous ECG is from one year ago, during the admission when he was diagnosed with pericarditis: 1 year ago ECG, with clinician and computer interpretatioin of pericarditis Normal 0 false false false EN-US X-NONE X-NONE What do you think?
He was started on a heparin drip and CTA of the chest was ordered to rule out pulmonary embolism. This is a case like many others posted (see list below) and the EKG from the patient’s original presentation can be quickly recognized as diagnostic for pulmonary embolism. In fact, Kosuge et al. Accessed May 28, 2024. This is a quiz.
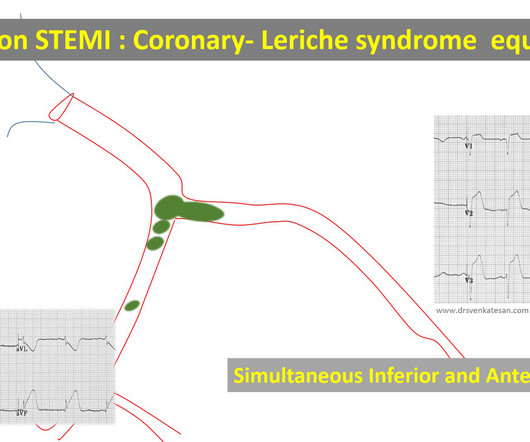
Embolic STEMI with showers of emboli into both LCX and LAD Simultaneous or sequential Anterior and Inferior STEMI 5. Mid or Proximal LAD lesion with proximal thrombus build-up Further possibilities Mimickers: Distal LAD lesions -Inferior ST elevation due to sparing of diagonal Wrong diagnosis -ERS pattern, pericarditis etc.
We have seen this pattern in many pts with acute right heart strain on this blog. __ Smith : The combination of T-wave inversion in V1-V3 and in lead III is very specific for acute pulmonary embolism. Acute pulmonary embolism was confirmed on CT: The patient did well with treatment. Unfortunately, we don't have those details.
She had idiopathic ventricular fibrillation in 1992, treated with an EPD (Picture 1A), later replaced by a transvenous ICD.She was diagnosed with left femoral deep venous thrombosis and bilateral pulmonary embolism and started on therapeutic anticoagulation. Despite empiric bronchial artery embolization, hemoptysis persisted.
Both of these are very suggestive of " No-Reflow ," or poor microvascular reperfusion due to downstream embolization of microscopic platelet-fibrin aggregates. MYOCARDIAL RUPTURE AND POSTINFARCTION REGIONAL PERICARDITIS KEY POINTS · Myocardial rupture occurs in 1 to 1.5% Myocardial Rupture and Postinfarction Pericarditis.
The morphology of V2-V4 is very specific in my experience for acute right heart strain (which has many potential etiologies, but none more common and important in EM than acute pulmonary embolism). CT angiogram showed extensive saddle pulmonary embolism. He had multiple cardiac arrests with ROSC regained each time. This is a quiz.
The combination of findings consistent with acute coronary occlusion in the anterior and inferior leads is likely due to a large "wraparound" LAD occlusion, should not be confused with the "diffuse" ST elevation of pericarditis, and will usually show reciprocal ST depression in aVL.
Patients with completed, transmural infarct are also at risk for post-infarction regional pericarditis and myocardial rupture. LV aneurysm puts them at risk for a mural thrombus, which puts them at risk for embolism, especially embolic stroke. Peak Troponin and Infarct Size: 60 ng/mL would be a very high first troponin.
This is a bad ST vector orientation, because it causes widespread STE and one of the most important mistakes that needs to be avoided here is thinking of the diagnosis of pericarditis. Such an out-of-proportion STE is virtually never seen in pericarditis. Look at the STE in lead II, aVF. Aslanger as one of the co-authors ).
They include myocardial ischemia, acute pericarditis, pulmonary embolism, external compression due to mass over the right ventricular outflow tract region, and metabolic disorders like hyper or hypokalemia and hypercalcemia. According to a recent systematic review and meta-analysis, spontaneous type 1 ECG had 2.4%
The "flu-like" illness suggests myo- or pericarditis, but that would be a diagnosis of exclusion. Then, part of the thrombus embolized into the LCx causing an inferoposterolateral OMI. (As Do not wait for the troponin; a lot of myocardium will be dead if you do. The case continues.
In this ECG Cases blog we look at 10 cases of patients with chest pain, including false positive STEMI, false negative STEMI, and other causes to help hone your ECG interpretation skills in time-sensitive cases where those very ECG skills might save a life.
CT angiogram chest: no aortic dissection or pulmonary embolism. Pericarditis? He spent several days in the PICU, undergoing workup including: Serial troponins: rising from 5,700 ng/L (unknown if I or T) to greater than 25,000 ng/L (greater than the lab's upper limit of reporting). No further troponins were measured.
CT pulmonary angiogram was negative for pulmonary embolism. If the patient continues to have reperfusion, then we would expect progressive terminal T wave inversion then full T wave inversion over time in the future ECGs. Second troponin T resulted at 1,318 ng/L. Chest x-ray was read as normal. Heparin was started. Reocclusion!
Angiogram: Severe 95% hazy distal LM Severe 80% ostial LAD, 100% occluded distal LAD thought to be due to distal embolization from the lesion in the proximal LAD. Post op chest pain Typical of post-op pericarditis (postpericardiotomy syndrome) There is ST Elevation in II > III, and STE in V3-5, but with flat T-wave.
The initial computer and final cardiology interpretation was a differential: “ST elevation, consider early repolarization, pericarditis, or injury.” But STEMI criteria ignore all this and look at ST segments in isolation. Based on STEMI criteria and unhelpful computer interpretation, the patient was rushed to the cath lab.
Smith : This is classic for pulmonary embolism (PE). Acute pulmonary embolism was confirmed on CT angiogram: The patient did well. See our other acute right heart strain / pulmonary embolism cases: A man in his 50s with shortness of breath Another deadly triage ECG missed, and the waiting patient leaves before being seen.
Despite apparently hearing the above history together with two diagnostic ECGs and a troponin compatible with OMI, the cardiologist thought the ECG represented pericarditis and recommended echocardiogram. Even if it is not atherosclerotic, young people can have embolic OMIs. The emergency physician consulted cardiology.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content