This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This ECG is diagnostic of anterior STEMI. This is a good sign for myocardialinfarction and does not happen in pericarditis. The distal inferior apical LAD was cut off by distal embolization from LAD culprit. The QRS is at least as important as the ST segment in diagnosing STEMI It has been constant since then.
Nature Reviews Cardiology, Published online: 02 April 2024; doi:10.1038/s41569-024-01020-2 In ST-segment elevation myocardialinfarction, the role of interventional modification of thrombi in the coronary arteries before stenting is controversial.
associated typical MyocardialInfarction therapies such as statins and ACE inhibitors with significantly decreased 1 year mortality in MINOCA patients, which suggests that they do indeed have a similar pathophysiology to MI patients with obstructive coronary disease. MINOCA I do not have the bandwidth here to write a review of MINOCA.
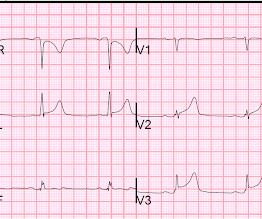
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
ng/mL (ULN = 0.030 ng/mL) , diagnostic of myocardial injury. The "criteria" for posterior STEMI are 0.5 Acute myocardial injury: Is it myocardialinfarction, or perhaps myocarditis? Is it STEMI or NonSTEMI? The troponin I returned at 4.1 mm STE in one lead. There is zero ST Elevation. This includes: 1.
This is a troponin I level that is almost exclusively seen in STEMI. In this case, profound shock for 1 hour would result in the same degree of infarction. A followup ECG was recorded 2 days later: No definite evidence of infarction. So this is either a case of MINOCA, or a case of Type II STEMI. Troponin I rose to 44.1
Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed Coronary Arteries). Transient and partial thrombosis at the site of a non-obstructive plaque with subsequent spontaneous fibrinolysis and distal embolization may be one of the mechanisms responsible for the occurrence of MINOCA. Learning Points: 1.
The ECG in ER is shown below: ECG is still diagnostic but we are watching the natural course of myocardialinfarction here. You may see a filling defect in distal LAD, most probably due to an embolization from proximal lesion. The lesion was successfully stented, but it was unfortunately done after a significant myocardial loss.
ng/mL This single initial troponin at this level, in the context of chest pain, is high enough to be diagnostic of acute myocardialinfarction. If there are T-wave inversions and elevated trops in the context of persistent pain, think of other pathologies such as pulmonary embolism. Her initial cTnI returned at 0.25
This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. But which myocardial walls are affected? However, by the time of the angiogram it had embolized distally, and had only done so after the right sided ECG was recorded. Can you tell from this ECG? The proposed mechanism is complex.
The limb leads have been removed because there was no ST elevation in those leads, the QRS complexes have been obscured because this is irrelevant to STEMI criteria, and red lines have been added to measure ST segment elevation. But STEMI criteria ignore all this and look at ST segments in isolation.
Smith , d and Muzaffer Değertekin a DIFOCCULT: DIagnostic accuracy oF electrocardiogram for acute coronary OCClUsion resuLTing in myocardialinfarction. Bi-phasic scan showed no dissection or pulmonary embolism. Take home messages: 1- In STEMI/NSTEMI paradigm you search for STE on ECG. Turk Kardiyol Dern Ars. 2021.21026.
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. In normal times, the most common use of cTni is in diagnosing, or ruling out, acute myocardialinfarction (AMI, a subcategory of acute myocardial injury.
Appearance of abnormal Q waves early in the course of acute myocardialinfarction: implications for efficacy of thrombolytic therapy. Both of these are very suggestive of " No-Reflow ," or poor microvascular reperfusion due to downstream embolization of microscopic platelet-fibrin aggregates. Raitt MH, et al. LV Thrombus , 1.5
They recorded this ECG: Obvious inferior STEMI/OMI What else? Here it is annotated in red: Our extremely smart radiologist, Gopal Punjabi , assures me that this finding can only be due to myocardialinfarction, not myocarditis. The patient was found to have an embolic source. Embolism with lysis. He called 911.
Note: the 2022 ACC Expert consensus Chest pain guidelines state that "posterior STEMI-Equivalent" is a sign of acute coronary occlusion. 2/3 of STEMI have a peak 4th generation troponin I greater than 10.0 Comment: The first ECG is diagnostic of OMI that does not meet STEMI criteria. NSTEMI-OMI").
The paramedics diagnosis was "Possible Anterolateral STEMI." LAD: type III-IV vessel with a proximal thrombotic or embolic occlusion (TIMI 0 flow). More proof that a huge STEMI may have normal or near normal initial troponin. Taken together, these findings suggest an ongoing extensive antero-lateral STEMI. Angiogram: 2.
The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI". No pulmonary embolism is identified. Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardialinfarction patients. Pain was decreased to 2/10.
Third, a slow motion segment showing delayed, brisk filling of the PDA due to dislodgment of a thrombus from contrast injection and distal embolization. A distal RCA lesion ( blue arrow ), Delayed brisk filling of an initially occluded PDA due to a thrombus dislodged during injection which embolized distally. SanzRuiz, R., Tang, Z.,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content