This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
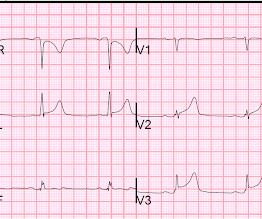
But there was some doubt as to whether it might be pericarditis because of the ST elevation in I and II, without ST depression in III. Add that to "sharp" pain and a 33 year old, and it is easy to convince yourself that this is, indeed, pericarditis. This is a good sign for myocardialinfarction and does not happen in pericarditis.
Appearance of abnormal Q waves early in the course of acute myocardialinfarction: implications for efficacy of thrombolytic therapy. Both of these are very suggestive of " No-Reflow ," or poor microvascular reperfusion due to downstream embolization of microscopic platelet-fibrin aggregates. The ECG in myocardial rupture 94.
This is a bad ST vector orientation, because it causes widespread STE and one of the most important mistakes that needs to be avoided here is thinking of the diagnosis of pericarditis. Such an out-of-proportion STE is virtually never seen in pericarditis. Considerations on the naming of myocardialinfarctions. 2019.09465.
The initial computer and final cardiology interpretation was a differential: “ST elevation, consider early repolarization, pericarditis, or injury.” Hyperacute T waves can be a useful sign of occlusion myocardialinfarction if appropriately defined. But STEMI criteria ignore all this and look at ST segments in isolation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










Let's personalize your content