This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Pulmonary embolism is the most common cardiovascular disease after myocardialinfarction and stroke. Konstantinides (Eur Heart J 41(4):543–603, 2020) Current guidelines categorize patients with PE as being at.
Prosthetic valve thrombosis (PVT) in aortic valve and its complication coronary embolism is a very rare condition. We present a young patient with acute myocardi. Diagnosis and treatment process is challenging.
We report a 42-year-old male patient who was diagnosed with acute myocardialinfarction (AMI), and subsequently underwent percutaneous coronary intervention (PCI) for revascularization. Then the patient experienced the most severe complications of IABP, including multiple organ embolism and intestinal necrosis.
Patients were stratified according to polygenic risk score tertiles and observed for the occurrence of ischemic stroke or systemic embolism, myocardialinfarction, and heart failure hospitalization. P=0.011) for ischemic stroke or systemic embolism, 1.15 (95% CI, 0.821.61;P=0.422) During a median followup of 4.6
ET Main Tent (Hall B1) - A Double-blind, Randomized Placebo Procedure-controlled Trial of an Interatrial Shunt in Patients with HFrEF and HFpEF: Principal Results From the RELIEVE-HF Trial - Empagliflozin After Acute MyocardialInfarction: Results of the EMPACT-MI Trial - CSL112 (Apolipoprotein A-I) Infusions and Cardiovascular Outcomes in Patients (..)
Nature Reviews Cardiology, Published online: 02 April 2024; doi:10.1038/s41569-024-01020-2 In ST-segment elevation myocardialinfarction, the role of interventional modification of thrombi in the coronary arteries before stenting is controversial.
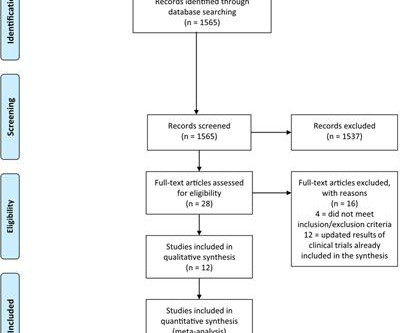
The pooled risks for overall response rate (ORR), 1-year progression-free survival (PFS), adverse events (AEs), immune-related AEs, (irAEs), hypertension, and vascular events defined as stroke, myocardialinfarction and pulmonary embolisms, were calculated.
COVID-19 likely increases relative risk (RR (95% CI)) of myocardialinfarction (3.3 (1.0 to 10)), pulmonary embolism (24.6 Other RTIs also likely increase the RR of myocardialinfarction (2.9 (95% to 11.0)), stroke (3.5 (1.2 to 44.9)) and deep venous thrombosis (7.8 (4.3 95% CI 1.8 to 4.9)) and stroke (2.6 (95%
TTE showed a reduced EF with multiple segmental abnormalities concerning for myocardialinfarction. A distinct feature of this case is the decompensation associated with ST elevation and segmental abnormalities, thought initially to be myocardialinfarction (MI), after an initial response to steroids.
Metadata was retrieved and transferred to bibliographic visualization software, VOSviewer, for co‐authorship and co‐occurrence analyses to identify trends in tenecteplase research.ResultsData visualization software identified three tenecteplase research clusters – myocardialinfarction, pulmonary embolism, and acute ischemic stroke.
Methods We retrospectively assessed whether compliance to the ‘1–3–6–12 days rule’ was associated with the composite endpoint (recurrent stroke, systemic embolism, myocardialinfarction, major bleeding or all-cause death).
BACKGROUND:Aortic arch plaques are associated with an increased risk of ischemic stroke in patients with cryptogenic stroke or prior embolic events. The primary outcome was ischemic stroke; the secondary outcome was combined cardiovascular events (ischemic stroke, myocardialinfarction, and cardiovascular death).
Pooled analysis of primary and secondary endpoints showed that apixaban significantly reduced the risk of stroke or systemic embolism by 47% (OR, 0.53(95%CI: 1.53), P=0.88), myocardialinfarction (OR, 0.97(95%CI: 1.53), P=0.88), myocardialinfarction (OR, 0.97(95%CI: 0.75), P<0.001), stroke by 44% (OR, 0.56(95%CI:
Ischaemic events were defined as myocardialinfarction, stroke, transient ischaemic attack or peripheral embolism at 1 year. We aimed to assess the accuracy of percutaneous coronary intervention (PCI)-derived models and the performance of a recalibrated model that included variables more applicable to TAVR.
Pooled analysis of primary and secondary endpoints showed that DOAC significantly reduced the risk of stroke or systemic embolism by 18% (OR, 0.82(95%CI: Pooled analysis of primary and secondary endpoints showed that DOAC significantly reduced the risk of stroke or systemic embolism by 18% (OR, 0.82(95%CI: years, respectively.
associated typical MyocardialInfarction therapies such as statins and ACE inhibitors with significantly decreased 1 year mortality in MINOCA patients, which suggests that they do indeed have a similar pathophysiology to MI patients with obstructive coronary disease. MINOCA I do not have the bandwidth here to write a review of MINOCA.
We used previously validated ICD-10-CM codes for acute ischemic stroke, intracerebral and subarachnoid hemorrhage, cerebral venous thrombosis, acute myocardialinfarction, pulmonary embolism, and acute deep venous thrombosis to define our study outcome.Results:We identified a total of 747 patients with OHSS in HCUP.
Oral anticoagulation also reduced a composite of cardiovascular death, all-cause stroke, peripheral arterial embolism, myocardialinfarction or pulmonary embolism (RR 0.85, 95% CI 0.73-1.00, The results from the two trials were consistent (I2statistic for heterogeneity=0%). 1.00, I2=0%; moderate-quality evidence).
BackgroundIn patients with acute cardiogenic cerebral embolism, a residual thrombus may still be present in the cardiac cavity even after reperfusion therapy. The secondary outcome was a composite end point event (cardiovascular death, nonfatal myocardialinfarction, nonfatal stroke) at 90 days.
This is a good sign for myocardialinfarction and does not happen in pericarditis. The distal inferior apical LAD was cut off by distal embolization from LAD culprit. Add that to "sharp" pain and a 33 year old, and it is easy to convince yourself that this is, indeed, pericarditis. However, look closely!
While intracardiac cardiac tumors and shunts are infrequent and typically asymptomatic, their existence can precipitate severe outcomes, including stroke, myocardialinfarction and sudden death.Case Description:A 69-year-old female presented with left sided facial droop, slurred speech and left arm weakness.
Appearance of abnormal Q waves early in the course of acute myocardialinfarction: implications for efficacy of thrombolytic therapy. Both of these are very suggestive of " No-Reflow ," or poor microvascular reperfusion due to downstream embolization of microscopic platelet-fibrin aggregates. Raitt MH, et al. the GISSI trial).
We assessed for interaction between age and discharge disposition and performed stratified analysis among patients aged < 65 years and older patients 65 years.Results:A total of 17 647 ICH patients alive at discharge (median age [IQR]: 69[57-79]; 45.2% female; 55.5% non-Hispanic White; 23.2% non-Hispanic Black; 10.4% Hispanic; 4.9%
Model fit was assessed using the Hosmer-Lemeshow test.Results:Among 142 eligible pre-ICH statin users (median age [IQR]: 77.5 [72-86] 72-86] years; 57.0% female; 66.0% non-Hispanic White [NHW]), 59 (41.6%) continued using statin post-ICH (median age [IQR]: 76 [73-85] years; 57.6% female; 69.5%
Adverse vascular outcomes used as endpoints include acute ischemic stroke, acute myocardialinfarction, deep vein thrombosis/pulmonary embolism, AF, and carotid artery dissection.A Patients with any adverse vascular outcomes before the index ECG were excluded. The mean age at the time of the index ECG was 44.3
The ECG in ER is shown below: ECG is still diagnostic but we are watching the natural course of myocardialinfarction here. You may see a filling defect in distal LAD, most probably due to an embolization from proximal lesion. The lesion was successfully stented, but it was unfortunately done after a significant myocardial loss.
However, AKI patients had higher rates of deep vein thrombosis (6.36% vs. 3.54%, p < 0.01), pulmonary embolism (4.22% vs. 1.42%, p < 0.01), pneumonia (21.39% vs. 8.84%, p < 0.01), urinary tract infection (19.07% vs. 13.32%, p < 0.01), sepsis (20.27% vs. 4.18%, p < 0.01), acute myocardialinfarction (12.14% vs. 3.21%, (..)
MINOCA: MyocardialInfarction in the Absence of Obstructive Coronary Artery Disease). pulmonary embolism, sepsis, etc.), Coronary thrombosis or embolism can result in MINOCA, either with or without a hypercoagulable state. I believe the latter (type II STEMI) is most likely. What is MINOCA? myocarditis).
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. In normal times, the most common use of cTni is in diagnosing, or ruling out, acute myocardialinfarction (AMI, a subcategory of acute myocardial injury.
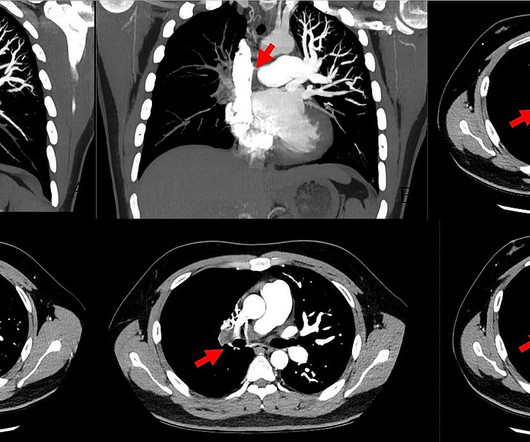
Smith , d and Muzaffer Değertekin a DIFOCCULT: DIagnostic accuracy oF electrocardiogram for acute coronary OCClUsion resuLTing in myocardialinfarction. Bi-phasic scan showed no dissection or pulmonary embolism. As his pain was very severe, emergency physicians concerned of aortic dissection and ordered a thoracic CT scan.
Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed Coronary Arteries). Transient and partial thrombosis at the site of a non-obstructive plaque with subsequent spontaneous fibrinolysis and distal embolization may be one of the mechanisms responsible for the occurrence of MINOCA. Learning Points: 1.
Acute myocardial injury: Is it myocardialinfarction, or perhaps myocarditis? The patient had been on a long drive, suggesting possible pulmonary embolism (this was unlikely given absence of tachyardia, hypoxia, or any other feature of PE), so we sent a d dimer. [We Is it acute or chronic? Is it STEMI or NonSTEMI?
And they of course activated the cath lab immediately, where he was found to have acute thrombotic occlusion (TIMI 0) of the proximal LAD, as well as embolic D1 occlusion. Instead, they reviewed the ECG immediately regardless of the computer interpretation of "normal." LCX and RCA were described as "normal" in the cath report.
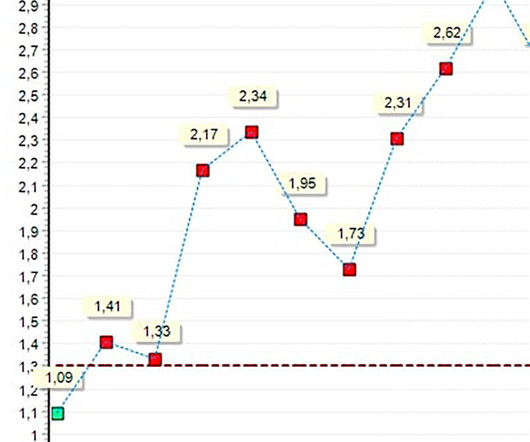
ng/mL This single initial troponin at this level, in the context of chest pain, is high enough to be diagnostic of acute myocardialinfarction. If there are T-wave inversions and elevated trops in the context of persistent pain, think of other pathologies such as pulmonary embolism. Her initial cTnI returned at 0.25
However, by the time of the angiogram it had embolized distally, and had only done so after the right sided ECG was recorded. The “bottom line” conclusions of their case report were that transient J waves may on occasion be induced by an acute injury current from impending myocardialinfarction.
Mid cavity obstruction in HCM is associated with apical aneurysm, systemic embolism, and arrhythmias. Thin posterior wall in inferior wall myocardialinfarction causing abnormal septal to posterior wall ratio can also cause suspicion of ASH. Doppler echo showing LVOT gradient in HCM.
The term MINOCA stands for Myocardialinfarction with non-obstructive coronary arteries. Coronary artery embolism – In this scenario, a blood clot which forms elsewhere goes down a coronary artery, causing a blockage but by the time we do the angiogram, the clot has dissipated and we see unobstructed vessels.
We used the Firth penalized likelihood method to perform a logistic regression, adjusted for age, sex, and history of myocardialinfarction to determine the association between high-risk embolic sources and AIS. For the primary analysis, we excluded patients with a history of atrial fibrillation.
AF is associated with an increased risk of death as well as multiple adverse outcomes, including stroke, cognitive impairment or dementia, myocardialinfarction, sudden cardiac death, heart failure (HF), chronic kidney disease (CKD), and peripheral artery disease (PAD). million.
Hyperacute T waves can be a useful sign of occlusion myocardialinfarction if appropriately defined. Accuracy of OMI ECG findings versus STEMI criteria for diagnosis of acute coronary occlusion myocardialinfarction. Acad Emerg Med 2023 3. Smith, Meyers. Ann Emerg Med 2023 4. Meyers, Bracey et al.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content