This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Up to 50% of patients with pulmonary embolism (PE) experience hemodynamic instability and approximately 70% of patients who die of PE experience an accelerated cascade of symptoms within the first hours of onset of symptoms, thus necessitating rapid evaluation and intervention. Journal of the American Heart Association, Ahead of Print.
Jesse MacLaren guides us through 10 cases of patients who present with generalized weakness or acute neurologic symptoms and discusses how to look for ECG signs of dysrhythmias, electrolyte emergencies, acute coronary occlusion, and demand ischemia in patients with generalized weakness and in patients with neurologic symptoms, to consider predisposing (..)
Many of the changes seen are reminiscent of LVH with “strain,” and downstream Echo may very well corroborate such a suspicion, but since the ECG isn’t the best tool for definitively establishing the presence of LVH, we must favor a subendocardial ischemia pattern, instead. Type I ischemia. Type II ischemia.
There is also STE in lead III with reciprocal depression in aVL and I, as well as some subendocardial ischemia pattern with STD in V5-V6 and STE in aVR. Aslanger's is a combination of acute inferior OMI plus subendocardial ischemia, and due to the ischemia vectors , it has STE only in lead III. Moreover, there is tachycardia.
In this phenomenon, a thrombus forms within the lumen of the stent graft component of the frozen elephant trunk prosthesis and puts the patient at risk for downstream embolization with visceral or lower limb ischemia. Therefore, the presence of ILT is associated with increased short-term mortality and morbidity.
We discover that for STEMI/OMI vs subendocardial ischemia, we should look for STEMI(-)OMI, subacute OMI, and OMI in the presence of LBBB and RBBB, and consider the differential for diffuse ST depression with reciprocal ST elevation in aVR.
CT of the chest showed no pulmonary embolism but bibasilar infiltrates. It should be kept in mind that on occasions, beta-one agonist can result in increased ventricular ectopy e.g., in severe myocardial ischemia (by increasing myocardial demand), or sometimes with congenital long-QT syndrome. She was intubated.
This usually represents posterior OMI, but in tachycardia and especially after cardiac arrest, this could simply be demand ischemia, residual subendocardial ischemia due to the low flow state of the cardiac arrest. This rules out subendocardial ischemia and is diagnostic of posterior OMI. V4-5 continue to show STD.
In terms of ischemia, there is both a signal of subendocardial ischemia (STD max in V5-V6 with reciprocal STE in aVR) AND a signal of transmural infarction of the inferior wall with Q wave and STE in lead III with reciprocal STD in I and aVL. The rhythm is atrial fibrillation. The QRS complex is within normal limits.
Previous studies have noted that ICAD-related LVOs, compared to embolic occlusions, have longer procedural times and lower successful reperfusion rates. Successful recanalization was defined as Thrombolysis in Cerebral Ischemia score ≥2b. However, clinical outcomes remain similar.
Neurological deficit score was measured.Results:The success rate in selectively embolized of ACA and MCA bifurcation was 93% (13 of 14 cases). Both fluoroscopy at 1, 3, 6, 24 h and TTC staining at 24 h after stroke model creation were performed. The median operating time was 7 min (interquartile range; 4-15 min).
We quantified PFO closure among individuals with ≥2 years of preprocedure coverage to establish indications, classified hierarchically as stroke/systemic embolism, migraine, transient ischemia attack, or other.Results:We identified 5315 patients undergoing PFO closure (51.8% underwent closure for stroke/systemic embolism, 10.2%
There is ST depression beyond the end of the wide QRS in I, II, aVF, and V4-V6, diagnostic of with subendocardial ischemia. It makes pulmonary embolism (PE) very likely. Eighth : STEMI even if from low flow, not ACS, can cause ischemia of the conduction system and result in complete AV block, even infra-HIS AV block. Summary: 1.
This may result in ischemia (lack of oxygen to the heart muscle), causing parts of the heart to weaken and enlarge. Blood Clots: An enlarged heart is more prone to developing blood clots, which can lead to stroke or pulmonary embolism.
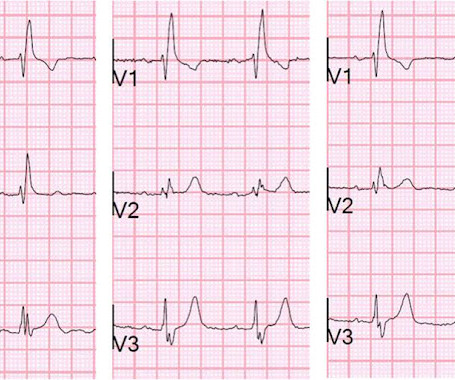
After resolution, there was T-wave inversion in V1-V3, highly suggestive of ischemia. There are features of the T-wave inversion, however, which argue against ischemia. Also, anterior ischemia is unlikely to spare lead V4 as in this case. This phenomenon is poorly understood, but involves "transient electrical remodeling."
He had a history of pulmonary embolism but was no longer on coumadin and states the pain is different. Here are V1-V3 from the last 3 ECGs: It is now clear that there is cardiac ischemia. 56 y/o male who presented with 12/10 severe chest pain starting at 3AM, radiating to his upper back. Wraparound? It was negative.
Normal RBBB, no evidence of ischemia. LV aneurysm puts them at risk for a mural thrombus, which puts them at risk for embolism, especially embolic stroke. In figure 3, I have inverted the image vertically to simulate recording leads from the opposite polarity (see Figure 3 ). R-waves of of normal height.
Often caused by sudden interruption of blood flow to the spinal cord due to embolic phenomena, intrinsic factors such as connective tissue disease, and due to intra/post‐operative hypotension leading to ischemia or infarction. IntroductionSpinal cord infarctions (SCI) are scarce entities, constituting only 0.3‐1%
The distal inferior apical LAD was cut off by distal embolization from LAD culprit. This is likely because 1) the ischemia to the inferior wall was only partial and 2) it reperfused quickly. The patient went to the cath lab and had an 80% occluded mid LAD with fresh thrombus. Lessons: 1.
We described a left intracranial ICA flow diversion occlusion without anterior circulation ischemia and left PCA ischemia demonstrated. There is concern that fragility of distal, smaller vessels may have an increased risk of procedural complications (e.g., arterial dissection and or perforations).
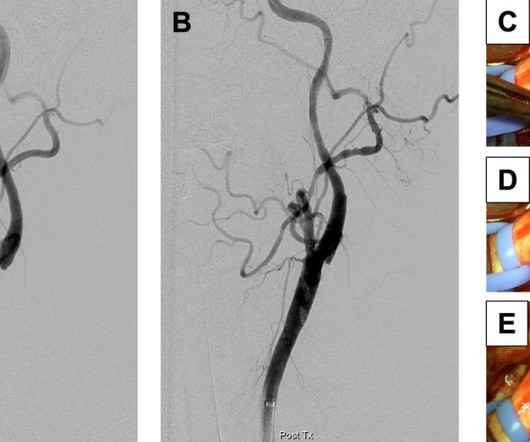
In his four months follow up clinic visit he had no further concerns of recurrent strokes or new symptoms.ResultsCarotid stump syndrome is a rare cause of cerebral and retinal ischemia; however, it must be considered in patients with recurrent ischemic strokes and chronic ipsilateral ICA occlusion.
remain hypo- or akinetic for some time even if not infarcted, just due to the profound ischemia incurred during the occlusive phase. Thus, an acute wall motion abnormality is not a sign of active or persistent ischemia, and thus is not necessarily an indication for emergent cath. Even many NOMI have wall motion abnormalities.
ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients.
This suggests further severe ischemia. Transient and partial thrombosis at the site of a non-obstructive plaque with subsequent spontaneous fibrinolysis and distal embolization may be one of the mechanisms responsible for the occurrence of MINOCA. Detailed coronary artery evaluation not performed. And yet the arteries remain open.
Low LV filling pressures are due to several etiologies, most commonly due to volume depletion (dehydration or hemorrhage), but also due to other etiologies including, but not limited to: mitral stenosis, pulmonary hypertension (chronic, or due to pulmonary embolism), or poor RV performance.
They include myocardial ischemia, acute pericarditis, pulmonary embolism, external compression due to mass over the right ventricular outflow tract region, and metabolic disorders like hyper or hypokalemia and hypercalcemia. According to a recent systematic review and meta-analysis, spontaneous type 1 ECG had 2.4%
However, by the time of the angiogram it had embolized distally, and had only done so after the right sided ECG was recorded. His astute observation is worthy of brief discussion: Rituparna et al document a case study report, in which J waves appeared to be induced by ischemia ( Pacing Clin Electrophysiol 30(6):817-819, 2007 ).
The bedside echo showed a large RV (Does this mean there is a pulmonary embolism as the etiology?) The flutter waves can conceal or mimic ischemic repolarization findings, but here I don't see any obvious findings of OMI or subendocardial ischemia. Here is his triage ECG: What do you think? Lots of info here. How about management?
Both of these are very suggestive of " No-Reflow ," or poor microvascular reperfusion due to downstream embolization of microscopic platelet-fibrin aggregates. More likely, the patient had crescendo angina, with REVERSIBLE ischemia for 48 hours that only became potentially irreversible (STEMI) at that point in time.
Use of objective evidence of myocardial ischemia to facilitate the diagnostic and prognostic distinction between type 2 myocardial infarction and myocardial injury. Clinically — despite an initial 2-fold increased troponin, the normal bedside Echo was reassuring against OMI or pulmonary embolism. Available from: [link] 9.
CT angiogram chest: no aortic dissection or pulmonary embolism. He spent several days in the PICU, undergoing workup including: Serial troponins: rising from 5,700 ng/L (unknown if I or T) to greater than 25,000 ng/L (greater than the lab's upper limit of reporting). No further troponins were measured.
Transient and partial thrombosis at the site of a non-obstructive plaque with subsequent spontaneous fibrinolysis and distal embolization may be one of the mechanisms responsible for the occurrence of MINOCA.
The outcome was arterial thromboembolism (ischemic stroke, embolism of extremity, or transient cerebral ischemia). Female sex was not considered a risk factor in any risk group.
Its characteristic cycle of ischemia, angiogenesis, and aberrant perfusion can lead to abnormal blood flow patterns that characterize the disease. The second most common treatment modality was endovascular embolization (36.9%). These studies consisted of 41 case reports, 6 case series, and 1 retrospective cohort study.
Evidence of acute ischemia (may be subtle) vii. Of the 67 patients who underwent targeted tests, suspected diagnoses were confirmed in 49 (73%) patients: aortic stenosis (n = 8, 1%), pulmonary embolism (n = 8, 1%), seizures/stroke (n = 30, 5%), and other diseases (n = 3). Left BBB vi. Pathologic Q-waves viii. LVH or RV d.
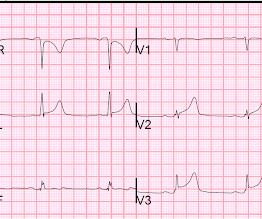
Smith : This is classic for pulmonary embolism (PE). Acute pulmonary embolism was confirmed on CT angiogram: The patient did well. See our other acute right heart strain / pulmonary embolism cases: A man in his 50s with shortness of breath Another deadly triage ECG missed, and the waiting patient leaves before being seen.
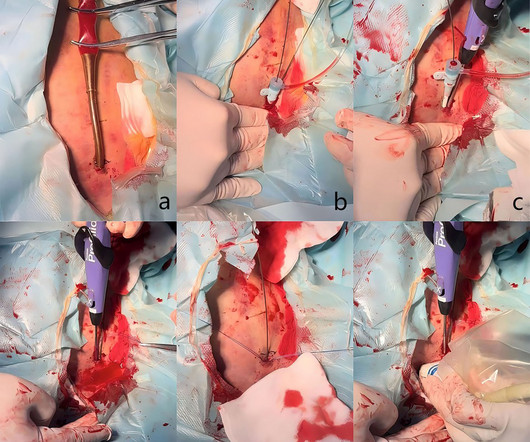
The complications associated with access included hemorrhagic events, pseudoaneurysm formation, limb ischemia, distal embolization, and wound infections.ResultsA total of 18 patients were included. The technical success was defined as achieving complete hemostasis without a bailout open repair. The median age of the cohort was 72.0
Management The web can create a flow disturbance, potentiating local thrombus formation, which can embolize producing resulting in cerebral ischemia. Fibromuscular hyperplasia of the carotid artery causing positional cerebral ischemia. J Neurointerv Surg. 2024 Nov 22;16(12):1294-1298. doi: 10.1136/jnis-2023-021243. Reference 1.Rainer
There is low voltage in the precordium which always makes reading ischemia harder. In ACS, chest pain is the warning sign of ongoing ischemia. Smith : As Willy says, and as we've said many times before, morphine will resolve pain without resolving ischemia. ECG 1 What do you think? To me, this ECG is not diagnostic.
Watch what happends as the heart recovers from its episode of ischemia. The ECG shows inferior ischemia. By itself seeing this ECG pattern does not necessarily mean that the patient has a pulmonary embolism. Are the T-waves in leads I and II hyperacute? Hard to tell. How can we know? By the evolution of the ECG!
Third, a slow motion segment showing delayed, brisk filling of the PDA due to dislodgment of a thrombus from contrast injection and distal embolization. A distal RCA lesion ( blue arrow ), Delayed brisk filling of an initially occluded PDA due to a thrombus dislodged during injection which embolized distally.
His initial high sensitivity troponin I returned at 1300 ng/L and given that his cardiac workup was otherwise unremarkable, a CT was obtained to evaluate for pulmonary embolism and aortic aneurysm or dissection but this too was unrevealing. Another EKG was also obtained. ECG at time 82 minutes: What do you think?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content