This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
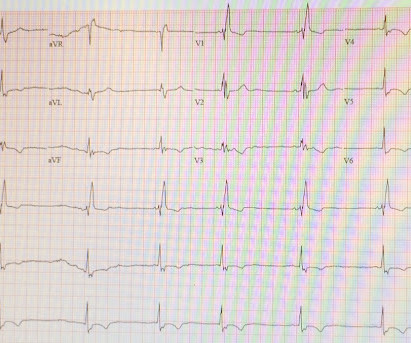
We have seen this pattern in many pts with acute right heart strain on this blog. __ Smith : The combination of T-wave inversion in V1-V3 and in lead III is very specific for acute pulmonary embolism. Acute pulmonary embolism was confirmed on CT: The patient did well with treatment. Unfortunately, we don't have those details.
Written by Pendell Meyers, edits by Smith: Case A 72 year old female with hypertension and COPD presented with sudden shortness of breath and chest pain. A new right bundle branch block in a sick patient with chest pain and/or shortness of breath is a worrisome finding concerning for LAD occlusion or significant pulmonary embolism.
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chest pain. Such an out-of-proportion STE is virtually never seen in pericarditis. Written by Emre Aslanger. Emre is a new Editor of the Blog.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. He was started on a heparin drip and CTA of the chest was ordered to rule out pulmonary embolism. What do you think?
The morphology of V2-V4 is very specific in my experience for acute right heart strain (which has many potential etiologies, but none more common and important in EM than acute pulmonary embolism). CT angiogram showed extensive saddle pulmonary embolism. He had multiple cardiac arrests with ROSC regained each time. This is a quiz.
Smith : This is classic for pulmonary embolism (PE). Acute pulmonary embolism was confirmed on CT angiogram: The patient did well. See our other acute right heart strain / pulmonary embolism cases: A man in his 50s with shortness of breath Another deadly triage ECG missed, and the waiting patient leaves before being seen.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












Let's personalize your content