This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Chronic Thromboembolic Pulmonary Hypertension (CTEPH) is a severe and complex condition that evolves from unresolved pulmonary embolism, leading to fibrotic obstruction of pulmonary arteries, pulmonary hypertension, and potential right heart failure.
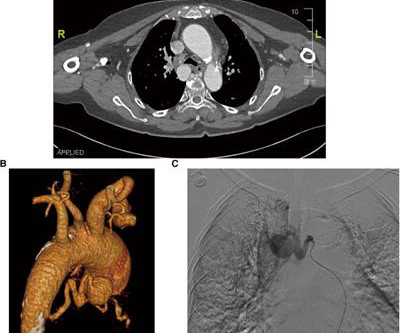
However, conventional surgical and transcatheter arterial embolization treatments are less effective. In the present case, a 76-year-old hypertensive woman was admitted with dizziness and diagnosed with an unruptured bronchial artery aneurysm, which was treated by transcatheter arterial embolization and aortic stent-graft.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. He was started on a heparin drip and CTA of the chest was ordered to rule out pulmonary embolism. What do you think?
The inflow aneurysms were accessed and embolized with coils using a second microcatheter prior to AVM embolization. Extensive but partial filling of the AVM was noted anteriorly but full embolization of the posterior aspect of the nidus was not achieved. Onyx‐18 was then injected into the main AVM pedicle under a blank roadmap.
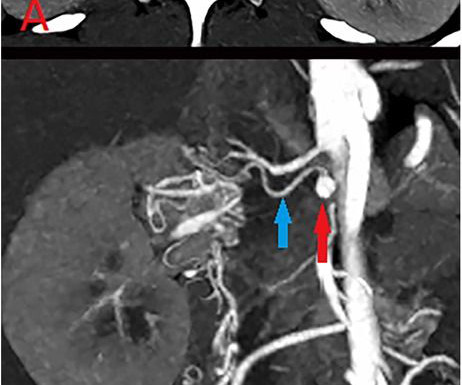
The left kidney function remained normal, allowing successful aneurysm embolization. Computed tomography angiography revealed a 2.2 mm mm left renal aneurysm and the absence of the left renal artery trunk, with collateral blood supply from the branch arteries of the aorta.
Six months later, the patient was evaluated by cardiology for hypertension diagnosed during hospitalization. Given ongoing embolic phenomena, likely from LSE, she underwent MVR with mechanical valve and LA appendage ligation and continued mycophenolate and warfarin. Cerebral angiogram further revealed FMD.
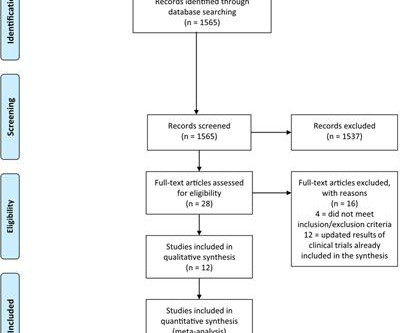
The pooled risks for overall response rate (ORR), 1-year progression-free survival (PFS), adverse events (AEs), immune-related AEs, (irAEs), hypertension, and vascular events defined as stroke, myocardial infarction and pulmonary embolisms, were calculated. In terms of efficacy, ICIs plus AIs achieved better ORR (OR 2.25, 95% CI: 1.70–2.97)
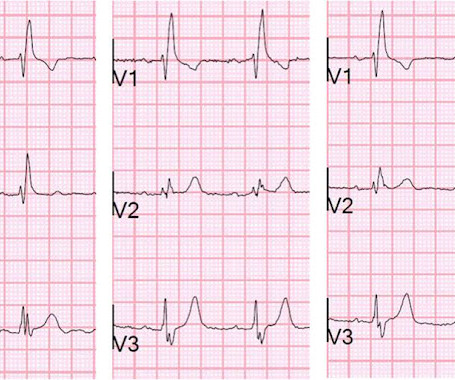
We have seen this pattern in many pts with acute right heart strain on this blog. __ Smith : The combination of T-wave inversion in V1-V3 and in lead III is very specific for acute pulmonary embolism. Acute pulmonary embolism was confirmed on CT: The patient did well with treatment. Unfortunately, we don't have those details.
Patients were stratified according to polygenic risk score tertiles and observed for the occurrence of ischemic stroke or systemic embolism, myocardial infarction, and heart failure hospitalization. P=0.011) for ischemic stroke or systemic embolism, 1.15 (95% CI, 0.821.61;P=0.422) During a median followup of 4.6
Clinical Cases and Poster Presentations The following list provides a brief look at the clinical cases and posters to be presented during the ACC Care of the Athletic Heart 2024 conference. All clinical cases and poster abstracts are embargoed until Thursday, June 6, 2024, at 1 p.m.
Written by Willy Frick with edits by Ken Grauer A woman in her 70s with a history of hypertension presented with acute onset shortness of breath. In patients with narrow QRS ( not this patient), this pattern is highly suggestive of acute pulmonary embolism. When EMS found her, she was dyspneic and diaphoretic.
For RV strain, acute vs chronic, we should look for signs of acute RV strain and chronic pulmonary hypertension. for low voltages we should consider pericardial effusion and other causes, and for hyperkalemia we should look for multiple signs of hyperkalemia as a guide for empiric calcium.
Specifically, this genetic factor was found to lower the risk of type 2 diabetes by 46.5%, coronary heart disease by 37.5%, ischemic stroke by 35.4%, cardiac-related mortality by 28.6%, heart failure by 28.2%, transient ischemic attack by 24%, atrial fibrillation by 15.2%, peripheral artery disease by 0.3%, and hypertension by 0.3%.
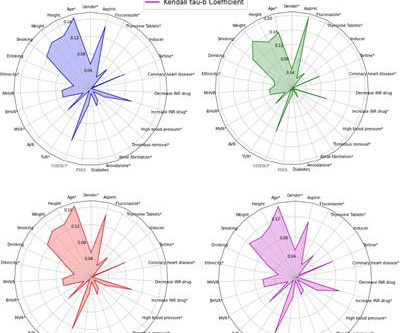
A relationship between hypertension, a history of severe preoperative embolism, and warfarin dose is found, which provides a useful reference for the warfarin dose administration in the future. mg/day, 0.13 mg/day), root mean square errors (0.18 mg/day, 0.20 mg/day) and R 2 (0.87, 0.82).
High Blood Pressure (Hypertension) Persistent high blood pressure forces the heart to work harder to pump blood. Chronic Pulmonary Disease Lung diseases like chronic obstructive pulmonary disease (COPD) can lead to pulmonary hypertension, which in turn can cause the right side of the heart to enlarge, a condition known as cor pulmonale.
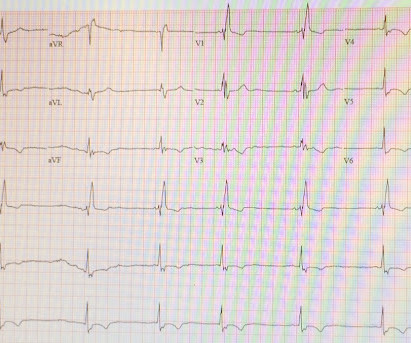
While new-onset LBBB might be indicative of acute coronary syndrome, RBBB may be associated with lung pathologies, pulmonary embolism, and pulmonary hypertension. Although RBBB is generally considered a relatively benign finding, recent data suggest an increased cardiovascular risk when detected in a general population [1].
Topic: Chronic thrombo embolic pulmonary hypertension.(CTEPH) This is a GIF run through of a recent presentation in PH seminar at Coimbatore, India. CTEPH) In this lecture, I have tried to highlight 1.Newer Newer definitions, Incidence and prevalence of CTEPH 2.The The pathologic transition phase between acute PE to CTEPH 3.Risk
IntroductionCerebral venous sinus thrombosis (CVST) presents diagnostic challenges, especially in its overlap with idiopathic intracranial hypertension (IIH). A cerebral angiogram showed a left occipital AV fistula, treated with onyx embolization. Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023.
male with pertinent past medical history including Atrial fibrillation, atrial flutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia.
About a fifth of all ischemic strokes are attributed to embolization of ruptured atherosclerotic plaque from carotid arterial stenosis. It has been mentioned that risk due to clonal hematopoiesis is equal in magnitude to conventional risk factors like smoking, hypertension, dyslipidemia and diabetes.
Smith comment: before reading anything else, this case screamed pulmonary embolism to me. CT chest showed left sided pulmonary embolism and a pulmonary infarct that had previously been mistaken for pneumonia. Past medical history included diabetes and hypertension. Vitals were normal.
He had a history of pulmonary embolism but was no longer on coumadin and states the pain is different. The patient was very hypertensive and had back pain, so they did a CT of his chest to rule out dissection. 56 y/o male who presented with 12/10 severe chest pain starting at 3AM, radiating to his upper back. Wraparound?
Often caused by sudden interruption of blood flow to the spinal cord due to embolic phenomena, intrinsic factors such as connective tissue disease, and due to intra/post‐operative hypotension leading to ischemia or infarction. IntroductionSpinal cord infarctions (SCI) are scarce entities, constituting only 0.3‐1%
BACKGROUND:Aortic arch plaques are associated with an increased risk of ischemic stroke in patients with cryptogenic stroke or prior embolic events. CONCLUSIONS:Aortic arch plaques may be a marker of cardiovascular risk rather than a direct embolic stroke source in older adults without prior stroke. Stroke, Ahead of Print.
Background:The STRACK project aims to improve post-stroke patient management and the transition from acute to primary care thanks to improvements in patient pathways and monitoring cardiovascular risk factors: heart failure, diabetes, atrial fibrillation, dyslipidemia and hypertension.
The morphology of V2-V4 is very specific in my experience for acute right heart strain (which has many potential etiologies, but none more common and important in EM than acute pulmonary embolism). CT angiogram showed extensive saddle pulmonary embolism. He had multiple cardiac arrests with ROSC regained each time. This is a quiz.
We performed a subgroup analysis among patients with embolic stroke of undetermined source (ESUS).Results:The Patients with atrial cardiopathy, compared to those without, were older (median age, 77 years versus 68 years), and more frequently had hypertension, coronary disease, and atrial fibrillation.
The bedside echo showed a large RV (Does this mean there is a pulmonary embolism as the etiology?) When you suspect pulmonary embolism due to large RV on POCUS, always look for right axis deviation and a large R-wave in V1 because the large RV may be entirely due to chronic RVH, not acute PE. Here is his triage ECG: What do you think?
Patients with a high risk of metabolic syndrome (>= 2 of the following: hypertension, diabetes, hyperlipidemia, or obesity) have a higher risk of AIS (1.37, 1.13 - 1.65), AMI (1.81, 1.19 - 2.75), and MACE (1.28, 1.13 - 1.44).Conclusions:Developing Results:Among 10,652 ICH patients (median age [IQR]: 70 [58 - 80] years; 47.7%
Notice I did not say "pulmonary embolism," because any form of severe acute right heart strain may produce this ECG. This includes, but is not limited to, PE, asthma/COPD exacerbation, hypoxic vasoconstriction from pneumonia, acute pulmonary hypertension exacerbation. Differences of Pulmonary Embolism T-waves from Wellens' T-waves: 1.
Strokes can be thrombotic, embolic or haemorrhagic. Stroke is a major cause of mortality, morbidity and economic burden. The key risk factor for cardioembolic stroke is atrial fibrillation or flutter, and oral anticoagulation (OAC) is recommended in all but the lowest-risk patients with evidence of these arrhythmias.
Postoperatively, the patient was hypertensive to a systolic blood pressure of 220 mmHg that was controlled with a nicardipine infusion that was gradually weaned off once the patient’s vitals were stable while in the Neuro‐ICU. There was no opacification of the aneurysms at the end of the procedure and no procedural complications (Figure 1D).
Adverse vascular outcomes used as endpoints include acute ischemic stroke, acute myocardial infarction, deep vein thrombosis/pulmonary embolism, AF, and carotid artery dissection.A Patients with any adverse vascular outcomes before the index ECG were excluded. total of 31301 patients (13783 MwA, 17518 MwoA) were included in our analysis.
Written by Pendell Meyers, edits by Smith: Case A 72 year old female with hypertension and COPD presented with sudden shortness of breath and chest pain. A new right bundle branch block in a sick patient with chest pain and/or shortness of breath is a worrisome finding concerning for LAD occlusion or significant pulmonary embolism.
Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chest pain. Chest Pain – Benign Early Repol or OMI? The culprit mid LAD lesion was stented.
ET Main Tent (Hall B1) Effect of Gamification, Financial Incentives or Both Combined to Increase Physical Activity Among Patients with Elevated Risk For Major Adverse Cardiovascular Events.
Low LV filling pressures are due to several etiologies, most commonly due to volume depletion (dehydration or hemorrhage), but also due to other etiologies including, but not limited to: mitral stenosis, pulmonary hypertension (chronic, or due to pulmonary embolism), or poor RV performance.
My answer: "This is classic for PE, but it can also be present in any hypoxia due pulmonary hypoxic vasoconstriction and resulting acute pulmonary hypertension and acute right heart strain. An ECG was texted to me (Smith) without any clinical information: What did I say? This is NOT Wellens. Is the patient hypoxic? The answer was yes.
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chest pain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. This is written by Willy Frick, an amazing cardiology fellow in St. He described it as "10/10" intensity, radiating across his chest from right to left.
The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis. The patient had been on a long drive, suggesting possible pulmonary embolism (this was unlikely given absence of tachyardia, hypoxia, or any other feature of PE), so we sent a d dimer.
in hypertensives are some of the features. Mid cavity obstruction in HCM is associated with apical aneurysm, systemic embolism, and arrhythmias. Hypertensive heart disease is an important differential diagnosis, but SAM is rare in this situation and there is evidence of greater diastolic dysfunction in HCM.
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chest pain. You may see a filling defect in distal LAD, most probably due to an embolization from proximal lesion. Written by Emre Aslanger.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content