This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
Distribution Variance of Focal Atrial Tachycardia Foci and Long-Term Outcomes After Ablation. ABSTRACT Introduction The distribution of the origin of focal atrial tachycardia (FAT) in patients with different ages have not been clearly elucidated.
BACKGROUND:Current outcomes from catheter ablation for scar-dependent ventricular tachycardia (VT) are limited by high recurrence rates and long procedure durations. Contrast-enhanced cardiac magnetic resonance images were used to reconstruct finite-element meshes, onto which regional electrophysiological properties were applied.
Abstract Introduction Understanding the spatiotemporal location of the spontaneous termination of ventricular tachycardia (VT) may provide new insights for ablation.
The ECGs show a wide complex, irregularly irregular tachycardia. The therapeutic and diagnostic cardiac electrophysiological uses of adenosine We can again see shortening of the PR interval and widening of the QRS complex with delta waves. On arrival to the ED, he was noted to be in a wide complex tachycardia with a rate in the 240s.
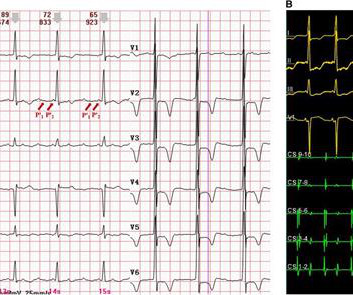
However, widely split P' waves in focal atrial tachycardia (AT) on a surface electrocardiogram (ECG) have rarely been reported. The electrophysiological mechanism is relatively difficult to clarify, requiring a electrophysiological study. Background Widely split P waves in sinus rhythm have been reported previously.
Using ECG recording and deductive reasoning, our teachers and predecessors classified the bradycardias and tachycardias and proposed many mechanisms, subsequently proven to be correct. Notwithstanding many insightful observations, the electrocardiogram (ECG) arguably ignited the big bang in our understanding of cardiac arrhythmias.
Ventricular tachycardia is a potentially life threatening cardiac arrhythmia. On the ECG, ventricular tachycardia can be defined as three or more ventricular ectopic beats occurring in a sequence at a rate more than 100 per minute. Another rare form of ventricular tachycardia is bidirectional ventricular tachycardia.
The aorta-mitral annulus conjunction (AMC) is uncommon site of origin of focal atrial tachycardias (AT). Hence, the electrophysiological and ablation target characteristics are poorly described.
There is limited data regarding safety, electrophysiologic characteristics and arrhythmia substrate during ventricular tachycardia (VT) ablation in patients with prior aortic valve replacement (AVR).
During atypical atrioventricular nodal reentrant tachycardia (AVNRT), the earliest atrial activation site following retrograde slow pathway (SP) conduction is at the atrial exit of the left inferior extension (LIE) in the coronary sinus (CS) or the right inferior extension (RIE) on the tricuspid annulus (TA).
ABSTRACT Atrial flutter (AFL), defined as macro-re-entrant atrial tachycardia, is associated with debilitating symptoms, stroke, heart failure, and increased mortality. Atypical AFL is a heterogenous group of re-entrant atrial tachycardias that most commonly occur in patients with prior heart surgery or catheter ablation.
Five criteria predict whether patients are likely or unlikely to have supraventricular tachycardia induced or ablated at an electrophysiologic study (EPS). They can be used as a guide for clinical decision making when considering invasive testing for patients with symptoms of tachycardia.
Establishing the precise mechanism of cardiac arrhythmias in the electrophysiology laboratory is one of the main requisites for a successful and safe ablation.
Hence, the electrophysiological and ablation target characteristics are poorly described. Focal AT at the aorta-mitral annulus conjunction (AMC) is uncommon.
The patient had undergone an electrophysiology study and radiofrequency ablation elsewhere and was subsequently referred to our centre. We found a narrow complex tachycardia of cycle 460 ms length ms which was repeatedly induced with atrial extrastimuli. What is the mechanism of the tachycardia?
The implications of ES on electrophysiological characteristics are not well understood. Ablation in VT in patients with electrical storm (ES) is challenging and associated with increased peri-procedural morbidity and mortality.
Epicardial Marshall bundle (MB) are frequently utilized in left atrial tachycardias (LATs) post atrial fibrillation (AF) ablation with pulmonary vein isolation and substrate modification.
Different types of recurrent atrial tachycardias (ATs) following Cox-Maze procedures have been reported, while biatrial tachycardia (BiAT) have not been systematically analyzed.
A 70-year-old male underwent an electrophysiologic (EP) study for episodic palpitations. Atrial extra stimulus testing induced a short- RP tachycardia initiated by prolongation of the AH interval. Baseline HV interval was 54 msec.
ABSTRACT Introduction Atrial tachycardias (AT) originating from the distal left atrial appendage (LAAd) are rare and pose significant challenges during catheter ablation. Electrophysiological study and activation mapping were performed, revealing a focal AT originating from the LAAd with a cycle length of 544ms (110bpm).
Very slow atrioventricular node reentry tachycardia (AVNRT) could compete with sinus rhythm giving the appearance of a non-reentrant accelerated junctional rhythm (AJR). Clinical awareness of very slow AVNRT masquerading as AJR is important because the former can be ablated with high success and low complications.
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. Complex ventricular tachycardias involving the fascicular system (fascicular ventricular tachycardias [FVTs]) can be challenging. To summarize, 5 cases had prior ablation with 2 previously misdiagnosed as supraventricular tachycardia.
Entrainment of ventricular tachycardia (VT) can be challenging as induction can lead to instability. Epicardial pace mapping has been described with multipolar coronary sinus (CS) catheters during electrophysiological studies, but not with a cardiac resynchronisation therapy (CRT) lead.
A 28-year-old man with recurrent palpitations and no structural heart disease presented with a documented wide QRS complex tachycardia (WCT). He had a history of slow pathway ablation for atrioventricular nodal reentrant tachycardia three months ago.
A 50-year-old woman was referred to our hospital for catheter ablation of a regular narrow QRS tachycardia with a short RP interval. In an electrophysiological study, the baseline atrio-His (AH) and His-ventricular intervals were normal. No retrograde dual atrioventricular (AV) nodal physiology was observed.
Atrioventricular nodal reentry tachycardia (AVNRT), identified as the most prevalent form of regular tachycardia in humans,3 exhibits a strong relationship with the anatomy and physiology of the AV node (AVN) and junction. Despite the temporal distance, Koch's triangle and pyramid remain a repository of unresolved mysteries.
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. During early childhood, 50% of patients develop multifocal atrial tachycardia, a treatment-resistant tachyarrhythmia of unknown pathogenesis. BACKGROUND:GermlineHRASgain-of-function pathogenic variants cause Costello syndrome (CS).
Studies have shown that mutations in the RYR2 gene, which encodes the RyR2 protein, are linked to several cardiac arrhythmias, including catecholaminergic polymorphic ventricular tachycardia (CPVT), long QT syndrome (LQTS), calcium release deficiency syndrome (CRDS), and atrial fibrillation (AF).
Managing scar-related ventricular tachycardia (VT) demands a nuanced understanding of the interplay between structural damage and electrophysiological function.
The patient was taken up for electrophysiology study during which a narrow complex tachycardia was induced which subsequently transformed into wide QRS tachycardia. What is the mechanism of the tachycardia? The 12 lead ECG (figure 1) and intracardiac recordings (figure 2) are shown below.
Anatomical and electrophysiological findings suggest the actual circuit of atrioventricular nodal reentrant tachycardia (AVNRT) involves the perinodal atrium. However, occasional instances where the atrium is dissociated from AVNRT have led to the concept of upper common pathways (UCP).
Atrial tachycardia (AT) originating from the left atrial appendage (LAA) is uncommon and the most difficult arrhythmia to eliminate. Therefore, we present the case of a 5-year-old girl with tachycardia-induced.
IntroductionFocal atrial tachycardia (FAT) is predominant in the pediatric population. A 12-lead electrocardiogram revealed a narrow QRS complex tachycardia with a rate of 157 beats per minute and a prolonged RP relationship. Echocardiography indicated a severely reduced ejection fraction of 22%.
Pulsed-field ablation (PFA) is becoming increasingly relevant in the field of electrophysiology. Data on the use is sparse, especially for atrial tachycardia (AT). Besides single-shot PFA devices for pulmonary vein isolation (PVI), point-by-point PFA is also gaining importance due to many possible applications.
ABSTRACT We encountered a single case in which a transition between orthodromic reciprocating tachycardia with a concealed nodoventricular pathway and atrioventricular nodal reentrant tachycardia with a bystander nodoventricular pathway was observed.
A 68 year-old man underwent diagnostic electrophysiologic study because of a symptomatic short RP supraventricular tachycardia (SVT). Transthoracic echocardiography was normal. Atrio-His (AH) and His-ventricular intervals measured 70ms and 55ms, respectively.
Torsades de Pointes (TdP) refers to a polymorphic ventricular tachycardia (VT) with undulating QRS axis that occurs in long QT syndrome (LQTS), although the term has been used to describe polymorphic ventricular tachyarrhythmias in which QT intervals are not prolonged, such as short-coupled variant of TdP currently known as short-coupled ventricular (..)
The 2019 ESC Guidelines for the management of patients with supraventricular tachycardia indicated that IV Amiodarone should not be considered in these populations. This electrophysiological property is called decremental conduction. More cases on WPW with atrial fibrillation : A young man with another episode of tachycardia.
Abstract Background The mechanism of typical slow-fast atrioventricular nodal re-entrant tachycardia (AVNRT) and its anatomical and electrophysiological circuit inside the right atrium (RA) and Koch's Triangle (KT) are not well known. The mean SR cycle length (CL) was 784.1 ± 6 ms and the mean tachycardia CL was 361.2 ± 54 ms.
1 Catheter ablation for atrial fibrillation (AF) and ventricular tachycardia (VT) has become the standard of care for many patients presenting with these arrhythmias.2–4 In the past decade, major advances were made in catheter ablation for arrhythmias and implantation of cardiac implantable electronic devices.1
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content