This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
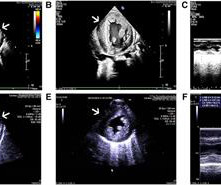
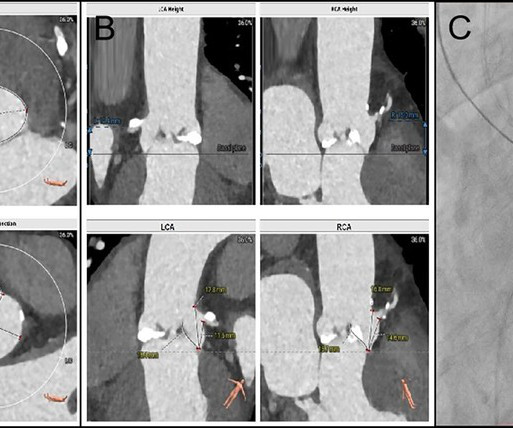
This comprehensive evaluation included the use of ultrasound echocardiograms, computed tomography (CT) scans, electrocardiograms, mutagenesis analysis, and structural analysis to gain insights into the patient's condition and the underlying mechanisms of PD.
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] Safety of computer interpretation of normal triage electrocardiograms. Hughes KE , Lewis SM , Katz L , Jones J. Acad Emerg Med.
Electrocardiogram (ECG) showed a prominent S wave in the left-sided leads and a prominent R wave in the right-sided chest leads, suggesting dextrocardia. An intravascular ultrasound was also performed, which was negative for vessel dissection. His vital signs were normal, and the physical examination was unremarkable.
Case continued A bedside ultrasound showed diminished LV EF and of course bradycardia. A 12-lead electrocardiogram, lead V4R , and leads V7-9 were recorded on admission. When narrow (above His bundle), it is likely to be atropine responsive. 1 mg of Atropine was given and the heart rate increased transiently to 60.
New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardial infarction in the emergency department. All electrocardiograms (ECGs) and coronary angiograms were blindly analyzed by experienced cardiologists. A emergent cardiology consult can be helpful for equivocal cases. Am J Med 2019, 132(5):622-630.
ALL TROPS WERE UNDETECTABLE A formal ultrasound was done: Normal estimated left ventricular ejection fraction at rest. The stress electrocardiogram is non-diagnostic. Normal estimated left ventricular ejection fraction improved with stress. No wall motion abnormality at rest. No wall motion abnormality with stress.
Intravascular ultrasound confirmed successful dilation of the coronary ostium. The patient experienced resolution of symptoms, and ventricular premature beats disappeared on electrocardiogram monitoring.
Moreover, electrocardiograms, which record the electrical activity of the heart, and wearable devices can provide artificial intelligence (AI) the data it needs to spot possible cases of valvular heart disease via fluctuations in heart rate, blood pressure, blood oxygenation and other factors.
My bedside ultrasound was of insufficient quality, but showed somewhat reduced overall EF, distended IVC without respiratory variation, no pericardial effusion, and diffuse bilateral B lines. == What do you think of her ECG? J Electrocardiol, 42 (2009), pp.
Santos Most Cited Article – Reduction in Hospitalization and Increase in Mortality Due to Cardiovascular Diseases during the COVID-19 Pandemic in Brazil Authors: Paulo Garcia Normando, José de Arimatéia Araujo-Filho, Gabriela de Alcântara Fonseca, Rodrigo Elton Ferreira Rodrigues, Victor Agripino Oliveira, Ludhmila Abrahão Hajjar, André Luiz (..)
Before the procedure, patients should have an electrocardiogram (ECG) and echocardiogram (ultrasound of the heart) to check the heart’s rhythm and function. Some patients need computed tomography or transoesophageal echocardiography to exclude the presence of a blood clot in the heart.
Check : [vitals, SOB, Chest Pain, Ultrasound] If the patient has Abdominal Pain, Chest Pain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. Abnormal ECG – looks for cardiac syncope.
tim.hodson Tue, 04/15/2025 - 15:06 April 1, 2025 UltraSight recently announced the presentation at the American College of Cardiology (ACC) Annual Meeting 2025 of three abstracts highlighting promising study findings using its AI-driven ultrasound platform. Bird, MD, cardiologist at Mayo Clinic. Listen to the episode here.
We aimed to determine the association between lesion-specific CAC score and stent underexpansion.MethodsIn this retrospective observational study, we included 416 lesions from 359 patients who underwent intravascular ultrasound (IVUS)-guided stent implantation. fold increased risk of stent underexpansion in NCCT cohort and 13.56-fold
A bedside cardiac ultrasound revealed grossly normal to hyperdynamic systolic function with no obvious areas of wall motion abnormalities. Fever not only unmasks a Brugada-type electrocardiogram (ECG) but also increases the risk of ventricular tachyarrhythmias such as ventricular fibrillation (VF) or sudden cardiac death.
Transthoracic echocardiogram, bilateral carotid Doppler ultrasound, and electrocardiogram were normal. No previous history of hypertension or diabetes. There was no abnormality in physical examination. Cranial magnetic resonance imaging and magnetic resonance angiography showed no abnormalities.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content