This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Electrocardiogram results showed sinus tachycardia, QRS widening, low-voltage complexes, and ST-segment elevation. A woman in her mid-20s presented with acute fever, chest pain, and exertional dyspnea. What would you do next?
This results in severe chest pain or discomfort, with the subsequent release of cardiac biomarkers, and alterations in the electrocardiogram. It can cause diminished heart function and mortality if not treated properly with suitable measures. Percutaneous Coronary Intervention was performed for 12.3% The average hospital stay was 8.51 (SD7.2)
Notwithstanding many insightful observations, the electrocardiogram (ECG) arguably ignited the big bang in our understanding of cardiac arrhythmias. Using ECG recording and deductive reasoning, our teachers and predecessors classified the bradycardias and tachycardias and proposed many mechanisms, subsequently proven to be correct.
Patients had routine 12-lead electrocardiograms (ECGs) regardless of presenting complaints. The most common presenting complaints and ECG abnormality were trauma (44%) and sinus tachycardia (15%), respectively. Two cardiology consultants blindly verified ECG findings.
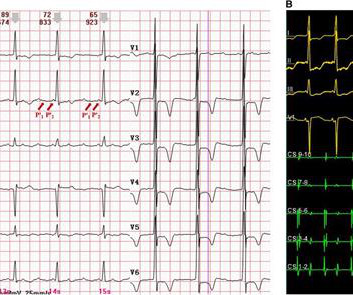
However, widely split P' waves in focal atrial tachycardia (AT) on a surface electrocardiogram (ECG) have rarely been reported. An electrophysiological study showed that the tachycardia arose from the left atrial appendage (LAA) and was conducted through two distinct pathways.
She was awake, alert, well perfused, with normal mental status and overall unremarkable physical exam except for a regular tachycardia, possible rales at both bases, some mild RUQ abdominal tenderness. Thus, I believe it is a regular, monomorphic, wide complex tachycardia. Or it could simply still be classic VT. What is the Diagnosis?
A twelve-lead electrocardiogram revealed atrial tachycardia (AT) with a cycle length of 240 ms. A 77-year-old male with a history of two catheter ablation procedures, including pulmonary vein isolation and superior vena cava (SVC) isolation, presented with symptomatic palpitations.
An electrocardiogram showed monomorphic ventricular tachycardia with a morphology suggesting right ventricular (RV) origin. A woman in her 90s presented to the emergency department with fever, hemoptysis, and syncopal episodes. What would you do next?
The electrocardiogram-based algorithm for predicting para-septal atrial tachycardia (PSAT) is limited by the significant overlaps in the P-wave morphology originating from various para-septal sites.
IntroductionFocal atrial tachycardia (FAT) is predominant in the pediatric population. A 12-lead electrocardiogram revealed a narrow QRS complex tachycardia with a rate of 157 beats per minute and a prolonged RP relationship. Echocardiography indicated a severely reduced ejection fraction of 22%.
Recognition of distinct arrhythmia syndromes over the last 3 decades, such as long QT syndrome, Brugada syndrome, catecholaminergic polymorphic ventricular tachycardia, and early repolarization (ER) syndrome (ERS), has changed this field, and the diagnosis of IVF has substantially decreased.1
In a world where technology reigns supreme, one of the most profound tools in medicine remains the irreplaceable electrocardiogram (ECG). Sinus tachycardia – sinus rhythm above 100 bpm is a sinus tachycardia. An abnormal electrocardiogram can mean many things. Usually does not exceed 160 bpm.
An otherwise healthy woman in her 20's with no past medical history presented with tachycardia. It can be managed with medications that convert atrial fibrillation to sinus, such as procainamide or ibutilide (and others), but when you have a wide complex very fast tachycardia, it is best to use electrical cardioversion.
Advanced arrhythmic substrate consisting of significant conduction abnormalities due to inflammation and fibrosis can be identified by specific electrocardiogram signs, such as fragmented QRS and ε wave. Among the ventricular tachycardia (VT) characteristics, multiple morphologies of monomorphic VTs (OR: 10.9,
Electrocardiographic imaging (ECGi) is a non-invasive technique for ventricular tachycardia (VT) ablation planning. In-silico pace mapping combines a personalized computational model with clinical electrocardiograms (ECGs) to generate a virtual 3D pace map. However, it is limited to reconstructing epicardial surface activation.
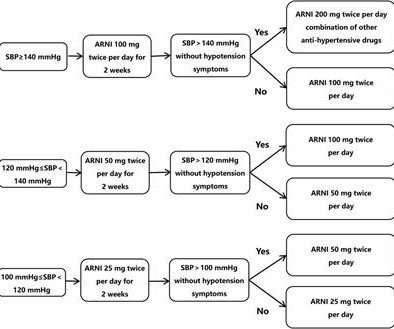
Sacubitril/valsartan can improve outcomes for patients with heart failure and ventricular tachycardia, but few studies examined whether it can reduce recurrence or improve cardiovascular outcomes in patients with persistent atrial fibrillation after catheter ablation.
Electrocardiogram (ECG) abnormalities can be found in almost all patients, with Wolff–Parkinson–White (WPW) syndrome being the most common. Case summary A 51-year-old woman with a 36-year history of intermittent palpitations was admitted due to hemodynamically stable ventricular tachycardia (VT).
Multifocal Atrial Tachycardia 2. A deep neural network for 12-lead electrocardiogram interpretation outperforms a conventional algorithm, and its physician over-read, in the diagnosis of atrial fibrillation. The rhythm is indeed irregularly irregular, so atrial fibrillation must be considered. Sinus with multifocal PACs 3. Poon et al.
He was not on any medication and his baseline electrocardiogram (ECG) was normal. A 44-year-old man with a structurally normal heart presented with a history of regular palpitations.
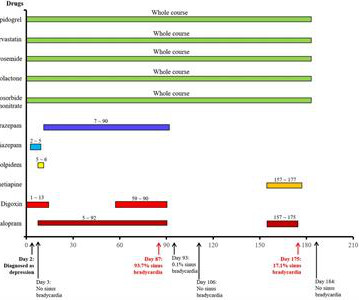
In an 82-year-old female patient with cardiac dysfunction using digoxin, tachycardia (average heart rate of 93 beats/min) was demonstrated by electrocardiogram (ECG). Here, a rare repeated sinus bradycardia event due to escitalopram is first reported.
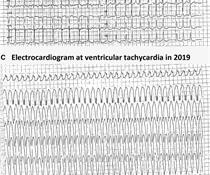
Electrocardiogram (ECG) showed sustained monomorphic VT at a rate of 160 bpm. Since its identification in 1981 its diagnosis has increased due to the advancements in cardiac imaging. It’s association with ventricular arrythmia (VA) and sudden cardiac death (SCD) underscores the importance of its identification.
A man in his 50s with recurrent palpitations, fatigue, and progressive exertion dyspnea had irregular narrow-QRS tachycardia in an incessant, repetitive fashion with heart rates up to 180 beats per minute and occasional short runs of wide-QRS tachycardia on Holter monitoring and 12-lead electrocardiogram.
An initial electrocardiogram (ECG) is provided below. While the initial impression might not immediately suggest ventricular tachycardia (VT), a closer examination raises suspicion. His current medication regimen includes apixaban, carvedilol, perindopril, spironolactone, torasemide, dapagliflozin, amiodarone, and ivabradine.
Ventricular arrhythmias during exercise can be documented in congenital long QT syndromes as well as in catecholaminergic polymorphic ventricular tachycardia. Bidirectional ventricular tachycardia is the classical arrhythmia noted in catecholaminergic polymorphic ventricular tachycardia.
Although sinus tachycardia is the most commonly encountered rhythmic disturbance, subsequent reports have highlighted other findings. Case presentation Here, we present the case of a 91-year-old woman with acute pulmonary embolism, whose initial electrocardiogram showed a complete atrioventricular block.
Abstract Introduction Typical atrial flutter (AFL) is a macroreentrant tachycardia in which intracardiac conduction rotates counterclockwise around the tricuspid annulus. The 12-lead electrocardiogram (ECG) and three-dimensional (3D) electroanatomical maps were analyzed.
Methods and Results A 21-year-old female with supraventricular tachycardia (SVT) and pre-excitation on electrocardiogram (ECG) underwent electrophysiology study (EPS) confirming an AS-AP with anterograde and retrograde conduction. Ablation in the NCC achieved immediate and persistent anterograde conduction block.
In that study commonest ECG abnormalites were QTc prolongation followed by brady/tachycardia and then ST segment deviations [3]. Lead electrocardiogram changes after supratentorial intracerebral hemorrhage. Lead electrocardiogram changes after supratentorial intracerebral hemorrhage. PMID: 7355693. Maedica (Bucur).
Notice there is tachycardia. I have warned in the past that one must think of other etiologies of ischemia when there is tachycardia. In this case, the patient had failed to take his atenolol in the AM and was having reflex tachycardia in addition to ACS. But we are now concerned with the precordial leads. BP was 160/100.
Electrocardiogram (ECG) and telemetry revealed junctional bradycardia with heart rate in 30s and sinus pauses (5-7 seconds). Patient did not report any symptoms and was hemodynamically stable. He was euvolemic on physical exam. Initial laboratory analysis was unremarkable. He was admitted for further workup of bradycardia.
An electrocardiogram is a machine used to record the heart's electrical activity. A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. Electrocardiogram, echocardiogram, and some other tests are done for patients with cardiac arrest. ECG and EKG refer to the same thing.
Follow-up contained regular visits at our outpatient clinic at 1, 3, 6, and 12 months including 7-day Holter electrocardiograms. ms after) and AF termination to atrial tachycardia (AT) or sinus rhythm (SR) in 12 patients (24%). Patients were mainly suffering from long-standing persistent AF (mean AF duration 50.30 ± 54.28
ECG in a person with persistent anginal pain for the past several hours showing significant ST segment depression anterolateral leads along with sinus tachycardia. Value of the electrocardiogram in localizing the occlusion site in the left anterior descending coronary artery in acute anterior myocardial infarction. J Am Coll Cardiol.
New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardial infarction in the emergency department. All electrocardiograms (ECGs) and coronary angiograms were blindly analyzed by experienced cardiologists. A slightly prolonged QTc ( although this is difficult to assess given the tachycardia ).
At the bottom of the post, I have re-printed the section on aVR in my article on the ECG in ACS from the Canadian Journal of Cardiology: New Insights Into the Use of the 12-Lead Electrocardiogram for Diagnosing Acute Myocardial Infarction in the Emergency Department Case 1. Updates on the Electrocardiogram in Acute Coronary Syndromes.
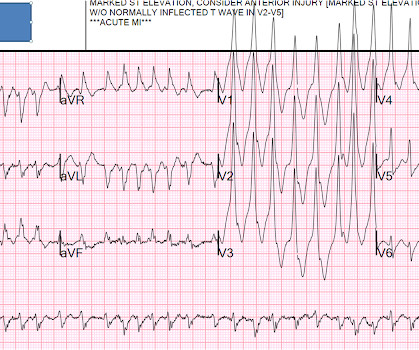
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. Induced Brugada-type electrocardiogram, a sign for imminent malignant arrhythmias. A rectal temperature was obtained which read 107.9 Heart Rhythm, 13(7): 1515-1520. [2]:
pre-existing, stable atherosclerosis) amidst any state of global duress – to include hypertension, hypoxia, tachycardia, hypotension, sepsis, and GI bleed, for example. New insights into the use of the 12 Lead Electrocardiogram for diagnosing Acute Myocardial Infarction in the emergency department. link] [1] Mirand, D.
You will note that it is essentially an unremarkable electrocardiogram except for some PACS. C linically — the rhythm we see in the long lead II of ECG #3 behaves similar to MAT, even though there is no tachycardia. This raised our concerns that the findings on his initial one were real.
There is sinus tachycardia and also a large R-wave in aVR. Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. Her temperature was 106 degrees. As part of the workup, she underwent an ECG.
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. Electrocardiogram-based risk stratification was useful in guiding the use of specialized cardiovascular tests. __ 9) François P.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content