This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
See these 2 articles Association between pre-hospital chest pain severity and myocardial injury in ST elevation myocardialinfarction: A post-hoc analysis of the AVOID study Author links open overlay panel [link] 1 Background We sought to determine if an association exists between prehospital chest pain severity and markers of myocardial injury.
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
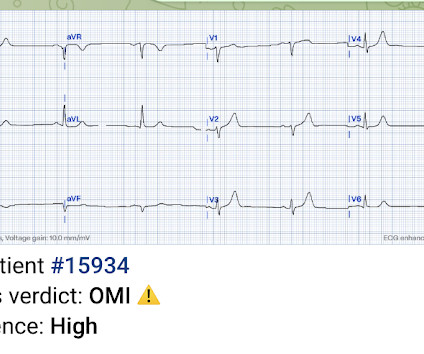
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
Their OMI Manifesto details how use of standard STEMI criteria results in an unacceptable level of inaccuracy, in which an estimated 25-30% of acute coronary occlusions are missed! The article by Aslanger, Smith et al that is featured above in today’s post has just been published.
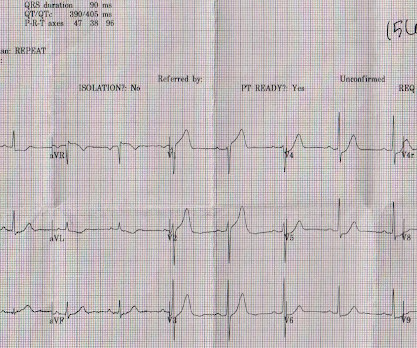
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. Zwolle MyocardialInfarction Study Group.
I believe there is not quite enough STE for formal STEMI criteria, but some might measure 1.0 mm of STE in II and III, or III and aVF, or V4 and V5, so some might say it fulfills STEMI criteria (remember, the interrater reliability of STEMI criteria is poor as shown in references below): McCabe et al.
The precordial ST-depression pattern on this ECG (and in this clinical setting) should immediately raise suspicion of Posterior STEMI! Posterior STEMI occurs in approximately 15-20% of acute MI, but the vast majority of the time it is seen in conjunction with inferior (Infero-Posterior) or lateral (Postero-Lateral) STEMI (1).
Precordial ST depression may be subendocardial ischemia or posterior STEMI. If you thought it might be a posterior STEMI, then you might have ordered a posterior ECG [change leads V4-V6 around to the back (V7-V9)]. So there was 3-vessel disease, but with an acute posterior STEMI. There is no ST elevation. See the list below.
There is an obvious inferior posterior STEMI(+) OMI. Literature cited In inferior myocardialinfarction, neither ST elevation in lead V1 nor ST depression in lead I are reliable findings for the diagnosis of right ventricular infarction Johanna E. What is the atrial activity? Is it sinus arrest with junctional escape?
This is diagnostic of inferior MI, though does not meet millimeter criteria for "STEMI." He was worried for inferior MI and ordered another, which was recorded 15 minutes later: Now clearly and obviously diagnostic of inferior STEMI. Unknown algorithm Interpretation: Inferior ST elevation, with reciprocal ST depression in aVL.
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
Introduction:Atrial fibrillation (AF), which can be easily identified through electrocardiogram (ECG), is a well-established predictor of ischemic stroke (IS) in comparison to other stroke subtypes. Stroke, Volume 56, Issue Suppl_1 , Page AWP317-AWP317, February 1, 2025. Analyses were conducted using R version 4.3.1.Results:In
You've read in my previous posts that I have a lot of evidence that Wellens' represents spontaneously reperfused STEMI in which the STEMI went unrecorded. New ST elevation diagnostic of STEMI [equation value = 25.3 Consequences of reocclusion after successful reperfusion therapy in acute myocardialinfarction.
As myocardialinfarction (MI) and many other diagnoses (for example left ventricular hypertrophy, prior MI etc.) can cause ST-segment elevation (STE) on electrocardiogram (ECG), the distinction between them may be hard and complicated.
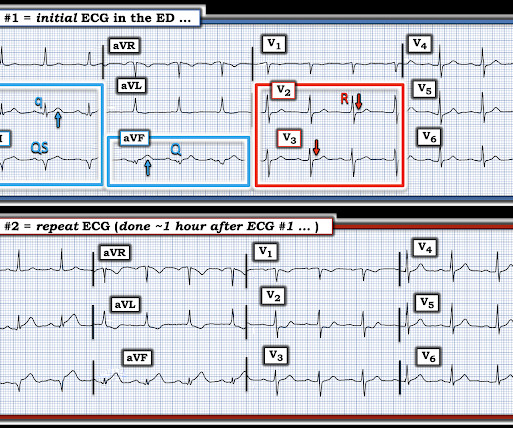
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. This confirms these Q waves are caused by an acute infarct. But the ECG still doesn’t meet STEMI criteria. Smith : Normal ST Elevation in V2-V4 never has an associated Q-wave! the computer interpretation 2.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI. New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardialinfarction in the emergency department.
Emergent cardiac outcomes in patients with normal electrocardiograms in the emergency department. Available from: [link] Excerpt: "To illustrate the limitations imposed by sample size, recent data from our institution reveal that we identify approximately 225 type I myocardialinfarctions (MI) in a typical year. Am J Emerg Med.
Relying on troponin elevation to diagnose acute coronary occlusion after at least 4 hours of infarction when the ECG can identify it immediately is poor choice. 3) STEMI criteria failed to identify this acute coronary occlusion, like many others. J Electrocardiology January–February, 2018; Volume 51, Issue 1, Pages e5–e6.
The limb leads have been removed because there was no ST elevation in those leads, the QRS complexes have been obscured because this is irrelevant to STEMI criteria, and red lines have been added to measure ST segment elevation. But STEMI criteria ignore all this and look at ST segments in isolation.
Smith , d and Muzaffer Değertekin a DIFOCCULT: DIagnostic accuracy oF electrocardiogram for acute coronary OCClUsion resuLTing in myocardialinfarction. His first electrocardiogram ( ECG) is given below: --Sinus bradycardia. Take home messages: 1- In STEMI/NSTEMI paradigm you search for STE on ECG. 2021.21026.
Safety of Computer Interpretation of Normal Triage Electrocardiograms. The cath lab was activated, as it should be with transient STEMI. See this case of transient STEMI: Spontaneous Reperfusion and Re-occlusion - My Bad Thinking Contributes to a Death. It is not yet available, but this is your way to get on the list.
You can see how V1, V2, aVR, and V4R would have ST elevation in either a right ventricular STEMI or with a septal STEMI, and how lateral leads, and even posterior leads, would have reciprocal ST depression. of patients with anterior STEMI, ST elevation of greater than or equal to 3.0 STE in V4R is confirmatory evidence.
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). LAFB, atrial flutter, anterolateral STEMI(+) OMI.
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
BP 142/100 HR 90 RR 16 (BBS CTA) SpO2 99 (RA) Dstick 110 My colleagues noted the ST-depression in the respective leads, as well, and STEMI activated to the nearest PCI center. 1] Here is the admitting ED ECG after cancellation of Code STEMI. The EMS crews were correct moving forward with STEMI activation. 1] Driver, B.
Appearance of abnormal Q waves early in the course of acute myocardialinfarction: implications for efficacy of thrombolytic therapy. cm diameter in the apex The presence of thrombus led the clinicians to state that this was a "late presentation STEMI." These do NOT indicate late, subacute MI. Raitt MH, et al. LV Thrombus , 1.5
LAD 80% mid LCx occluded mid (acute infarct lesion) RCA 80% mid. PCI mid LCx So this is an OMI (Occlusion MyocardialInfarction), but not a STEMI Echo: Decreased left ventricular systolic performance, mild/moderate. Cardiac Troponin Changes to Distinguish Type 1 and Type 2 MyocardialInfarction and 180-Day Mortality Risk.
The utility of the triage electrocardiogram for the detection of ST-segment elevation myocardialinfarction. link] In this paper, in a department in which they state they have only 50 STEMI per year, they looked at only 8 days worth of triage ECGs for a total of 538. Am J Emerg Med 36(10):1771-1774. October 2018.
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
His father and brother both died of myocardialinfarction at ages 61 and 45, respectively. STEMI was activated and the patient went to Cath on arrival. New insights into the use of the 12 Lead Electrocardiogram for diagnosing Acute MyocardialInfarction in the emergency department. 2] Aslanger, E.,
Here is the PMcardio Queen of Hearts interpretation of the ECG: STEMI equivalent detected. Inferior and posterior OMI without STEMI criteria. About an hour later another ECG was obtained: Barely meets STEMI criteria in inferior leads, but obvious inferior and posterior OMI. The cath lab was now activated for STEMI.
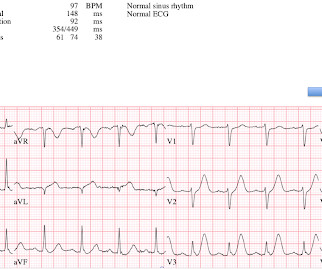
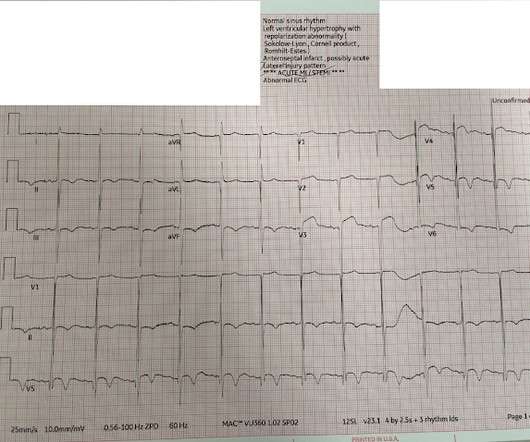
Even before we have clinical context, this ECG simply does not appear concerning for OMI, notwithstanding the machine's interpretation ** ** ACUTE MI / STEMI ** **. But in the world of STEMI, this is a challenging ECG to most. Artificial intelligence (AI) algorithms show promise to improve electrocardiogram (ECG) interpretation.
The de Winter electrocardiogram pattern is an infrequent presentation, reported to occur in 2% to 3.4% of patients with anterior myocardialinfarction ( 1 ). This ECG pattern is my favorite example of how the STEMI criteria are fundamentally flawed. We have a series of 20 TIMI-0 LAD Occlusions that do meet STEMI criteria.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content