This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
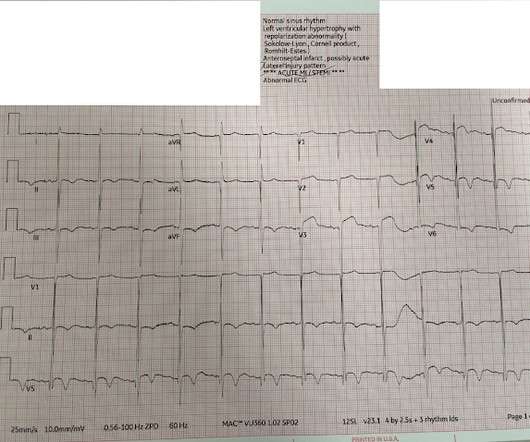
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. Hence the first ECG was labeled 'anterior ischemia' based on ST depression, rather than identifying this as reciprocal from posterior OMI. But are there any other signs of Occlusion MI? Meyers et al.
Myocardialischemia may induce myocardial fibrosis, a condition that progressively leads to ventricular remodeling, heightening the risk of heart failure. The timely detection of myocardial fibrosis is crucial for intervention and improved outcomes. The results demonstrated tracer-specific uptake (SUVmax = 4.6)
The Kardia 12L ECG System, featuring a game-changing patented technology, is the world’s first AI-powered handheld 12-lead electrocardiogram ( ECG ) system with a unique single-cable design. This is the world’s first AI that can detect life-threatening cardiac conditions, including heart attacks, using a reduced leadset.
See these 2 articles Association between pre-hospital chest pain severity and myocardial injury in ST elevation myocardialinfarction: A post-hoc analysis of the AVOID study Author links open overlay panel [link] 1 Background We sought to determine if an association exists between prehospital chest pain severity and markers of myocardial injury.
Mechanism is thought to be due to sustained sympathetic stimulation, probably caused by dysfunction of insular cortex resulting in reversible neurogenic damage to the myocardium which could include contraction bands and subendocardial ischemia [2]. Lead electrocardiogram changes after supratentorial intracerebral hemorrhage.
Precordial ST depression may be subendocardial ischemia or posterior STEMI. I have warned in the past that one must think of other etiologies of ischemia when there is tachycardia. Whether it is subendocardial ischemia or posterior STEMI, if you cannot get it to resolve, you must activate the cath lab. There is no ST elevation.
5] Back to the case The patient had serial ECGs over the next hour with no significant change: The first troponin came back at 1,400 ng/L (normal <26 in males and <16 in females), confirming MI – and the patient’s refractory ischemia indicated this was an Occlusion MI. Clin Cardiol 2022 4. Herman, Meyers, Smith et al.
Computer read: "Non-specific ST abnormality, consider anterior subendocardial ischemia" There are very poor R-waves in V1-V4 suggesting old anterior MI. Firstly, subendocardial ischemia does not localize on 12-Lead ECG. But the real question at hand is: Are these precordial ST-depressions a result of subendocardial ischemia?
The ECG in the chart was read as "no obvious ST changes," (even though no previous ECG was available) and the formal read by the emergency physicians was: "ST deviation and moderated T-wave abnormality, consider lateral ischemia." Consequences of reocclusion after successful reperfusion therapy in acute myocardialinfarction.
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
hours later, after PCI: There is a significant QS-wave in V2, with some persistent ST elevation, suggesting incomplete small vessel reperfusion and significant infarction. The patient continued to have ischemia after PCI, and in fact had an episode of polymorphic VT shortly after while in the ICU. This was recorded 2.5
ST segment elevation in aVR in proximal LAD occlusion before first septal is thought to be due to transmural ischemia of the basal part of the septum. Value of the electrocardiogram in localizing the occlusion site in the left anterior descending coronary artery in acute anterior myocardialinfarction. J Am Coll Cardiol.
There is broad subendocardial ischemia as demonstrated by STE aVR with concomitant STD that almost appears appropriately maximal in Leads II and V5. There is LBBB-like morphology with persistent patterns of subendocardial ischemia. This is the initial ECG: The QRS is widened with a regular cadence, and there are no discernable P waves.
Background: The value of the 12-lead ECG in the diagnosis of non-ST-elevation myocardialinfarction (NSTEMI) is limited due to insufficient sensitivity and specificity of standard markers of ischemia and because ECG confounders may prevent their application.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" That said, complete LM occlusion would be expected to have subepicardial ischemia (STE) in these myocardial territories: STE vector 1.
His father and brother both died of myocardialinfarction at ages 61 and 45, respectively. There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1]
Diagnosis of Acute MyocardialInfarction in the Presence of Left Bundle Branch Block using the ST Elevation to S-Wave Ratio in a Modified Sgarbossa Rule. Electrocardiographic Diagnosis of Acute Coronary Occlusion MyocardialInfarction in Ventricular Paced Rhythm Using the Modified Sgarbossa Criteria.
When “spot diagnosing” precordial ST-depression I instinctively evaluate aVR for any corresponding ST-elevation to see if an emerging pattern of broad subendocardial ischemia can be appreciated, in which the ST-depression should be otherwise global and demonstrably maximal in Leads II and V5. ST-elevation, etc.) is present. 1] Driver, B.
LAD 80% mid LCx occluded mid (acute infarct lesion) RCA 80% mid. PCI mid LCx So this is an OMI (Occlusion MyocardialInfarction), but not a STEMI Echo: Decreased left ventricular systolic performance, mild/moderate. Cardiac Troponin Changes to Distinguish Type 1 and Type 2 MyocardialInfarction and 180-Day Mortality Risk.
Appearance of abnormal Q waves early in the course of acute myocardialinfarction: implications for efficacy of thrombolytic therapy. More likely, the patient had crescendo angina, with REVERSIBLE ischemia for 48 hours that only became potentially irreversible (STEMI) at that point in time. Raitt MH, et al. Methods: Oliva et al.
HIV and Cardiovascular Disease: HIV infection itself is associated with an increased risk of cardiovascular disease and can double the risk of CVDs, including myocardialinfarction and stroke. Plus, abacavir, an NRTI, has been linked to an increased risk of myocardialinfarction.
She requires maximal medical management per all current guidelines (including heparin and P2Y12 inhibitor per cardiology), as well as consideration for emergent cath in the case of persistent ischemia. So what will you do for this patient? They found an acute, total, thrombotic occlusion of the proximal LAD. They opened it. Patel et al.,
Abnormal Electrocardiogram (ECG): Defined (San Fran syncope rule) as any new changes when compared to the last ECG or presence of non-sinus rhythm. Evidence of acute ischemia (may be subtle) vii. to 1.64) for myocardialinfarction or death from coronary heart disease, and 1.06 (95 percent confidence interval, 0.77
The de Winter electrocardiogram pattern is an infrequent presentation, reported to occur in 2% to 3.4% of patients with anterior myocardialinfarction ( 1 ). Tall precordial T waves with depressed ST take-off: an early sign of acute myocardialinfarction? Transient ischemia may lead to "stunning".
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content