This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This patient could have very easily been overlooked, both because the ECG was STEMI negative and because the Q waves were attributed to an “old infarct”. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion. OMI or STEMI? As cardiology documented, “possible STEMI.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. This case is an example of the steps we can all take in daily practice as the paradigm shifts from STEMI to OMI.
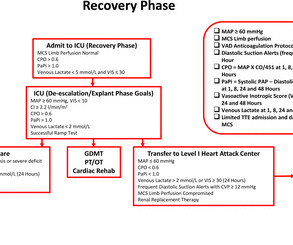
Methods and analysis The Durango model is a prospective single-centre registry designed to enable early identification of patients with STEMI-CS to facilitate primary reperfusion therapy with a shock team management algorithm in a rural level II heart attack centre.
The Minneapolis Heart Institute Foundation (MHIF) is presenting leading research focused on trends in ST-elevation myocardial infarction (STEMI), the most severe form of a heart attack, at the American College of Cardiology’s Annual Scientific Session (ACC.24), 24), being held April 6-8 in Atltanta, GA.
MY Thoughts on Today's CASE: As important as providing a brief, relevant history is for optimal clinical ECG interpretation — Cases like the one today often prove even more educational, because we are not given any history ( and therefore need to deduce the most likely clinical setting to explain the ECG in front of us ).
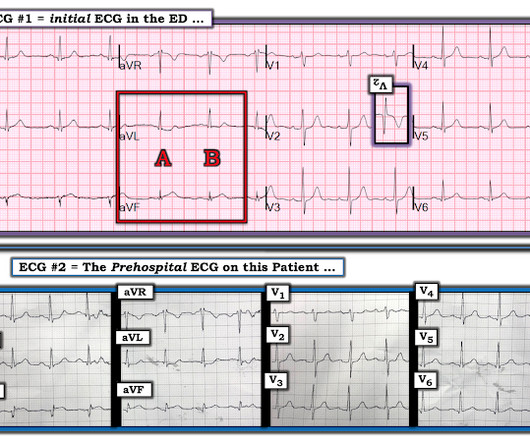
This was sent by : Jacob Smith, DO Emergency Medicine Resident Ohio Health Doctors Hospital Emergency Residency Christopher Lloyd, DO, FACEP Director of Clinical Education, USACS Midwest Case A 30 year old patient presents to triage with chest pain. This is diagnostic of inferior MI, though does not meet millimeter criteria for "STEMI."
So there is definitely no STEMI, and the STE is normal. But after reading this blog, you all know that most OMI do NOT meet STEMI criteria. Bedside echo revealed anteroseptal wall motion abnormality at which point I activated a code STEMI. mm in men over age 40. So the computer is correct in calling it normal.
One more remote risk in CTO is, acute collateral shutdown causing STEMI/NSTEMI. link] Post-amble Living with a single coronary artery, is potentially a frightening scenario for the patient* which has to supply its own area and also, need to donate the occluded coronary artery. What will happen if a single donor (RCA/LCX) gets closed?
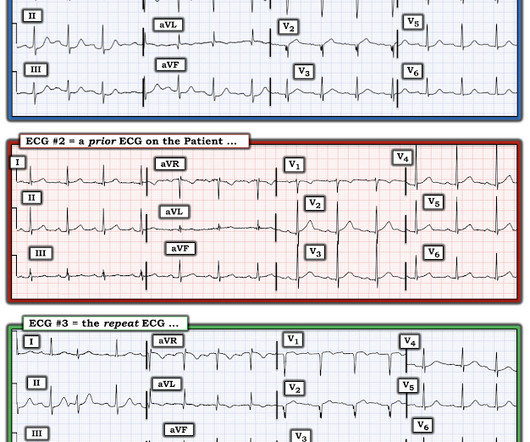
This algorithm called it a STEMI. Yet it gave a diagnosis of STEMI. This is, in effect, a transient STEMI 2. For educational purposes — I think it helpful to initially interpret ECG #1 as if it was the only ECG available in this case, keeping in mind that this patient’s chest pain had resolved at the time ECG #1 was recorded.
Is this inferor STEMI? Atrial Flutter with Inferior STEMI? Christmas Eve Special Gift!! Prehospital Cath Lab Activation: What do you think? Global ST depression with ST elevation in aVR - what is the cause? Tachycardia and ST Elevation. Atrial Flutter Mimicking ST Depression What is the Diagnosis?
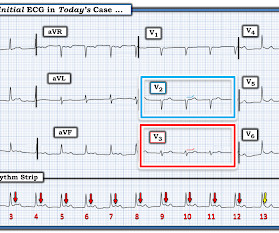
Guaranteed , it will take no more than 3 seconds for your "educated eye" to begin the interpretation of each and every ECG you are given with a QUICK SCAN of the long lead II rhythm strip under the 12-lead — in order to assess IF each QRS complex is preceded by an upright P wave with a constant PR interval.
In addition to educational insights — Dr. Nossen's contributions periodically serve as a source for review of the Cabrera Format , recorded at 50 mm/second — as is the customary ECG recording format in his country.
Anterior STEMI? T-wave inversions and dynamic ST elevation Tachycardia, hyperthyroid, and ST elevation. What is it? 2 Cases of Resolved Chest Pain with Dynamic Terminal T-wave Inversion Is it Wellens' Syndrome? Activate the Cath Lab?
Written by Jesse McLaren, with edits from Meyers Four patients presented with chest pain or shortness of breath, and ECGs labeled ‘inferior STEMI’. Less concavity associated with hyperacuity This can help identify false negative STEMI, or STEMI(-)OMI, at risk for delayed reperfusion. More asymmetry 3.
I was using this post (below) to educate my scribe, maybe Ill send to the cardiologist, if Im feeling brave" 7 steps to missing posterior Occlusion MI, and how to avoid them. Here is the Queen of Hearts interpretation: Here is the cardiologist's impression: "EKG does not show a STEMI." They do not recognize these patterns.
EKG interpretation skills have little to do with one's level of education. In fact, much of what passes for EKG education can actually harm one's interpretation skills. Written by Hans Helseth Hans is an EKG tech who is applying to medical school. 5 years later ( now in 2025 ) the problem remains.
Here is the Queen of Hearts interpretation, appropriately reading STEMI equivalent, highlighting anterior and lateral leads with explainability, and even detecting reduced LVEF. The Cardiologist stated that the ECG did not show signs of STEMI, but rather NSTEMI, recommended serial ECGs and troponins, and cancelled the activation request.
link] == MY Comment , by K EN G RAUER, MD ( 1/20 /2025 ): == If you Google, Broken Heart Syndrome you will immediately see reference to many pages of Patient Education news briefs and informationals, in which the questions addressed are, Can You Really Die of a Broken Heart? Circulation , 145 (13), 10021019.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content