This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background Percutaneous coronary intervention (PCI), the preferred coronary reperfusion strategy, induces endothelial trauma which may mount an inflammatory response. This has been shown to increase the likelihood of further major adverse cardiovascular events (MACE). Colchicine, a cheap and widely used anti-inflammatory has shown promise in improving cardiovascular outcomes.
What is the preferred order of vasopressors and ionotropes in the management of cardiogenic shock? In which patients would dobutamine be preferred over milrinone and vice versa? How can we best pick up occult cardiogenic shock before it floured shock kicks in? What are the best strategies to efficiently get the patient in cardiogenic shock to definitive care, whether that be the cath lab or the operating room?
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chest pain. What do you think? Sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. There’s primary ST depression in the precordial leads maximal in V3-4, and an inverted T wave in V2.
In the last few years, we’ve witnessed a massive transformation in analytics in the cardiology department. No longer it’s only about digital dashboards, but technology is transforming all areas in Cath labs. One of the prime examples is Cath Lab Software. Such Cath lab solutions have had a disruptive impact as they provide a new way to mine relevant data, ensure quality, and pave the way for better overall management.
Speaker: Simran Kaur, Co-founder & CEO at Tattva Health Inc.
AI is transforming clinical trials—accelerating drug discovery, optimizing patient recruitment, and improving data analysis. But its impact goes far beyond research. As AI-driven innovation reshapes the clinical trial process, it’s also influencing broader healthcare trends, from personalized medicine to patient outcomes. Join this new webinar featuring Simran Kaur for an insightful discussion on what all of this means for the future of healthcare!
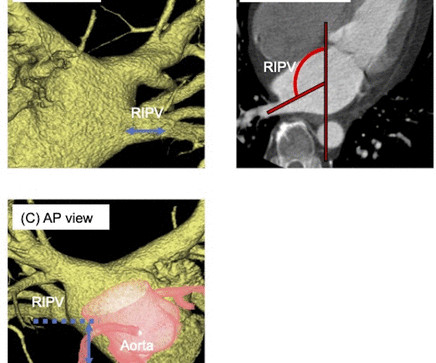
Background The limited availability of balloon sizes for cryoballoon leads to anatomical limitations for pulmonary vein (PV) isolation. We conducted a comprehensive systematic analysis on procedural success rate, atrial fibrillation (AF) recurrence rate and complications of cryoballoon ablation in association with the anatomy of the left atrium and PV based on preprocedural CT to gain insights into proper treatments of patients with AF using cryoballoon.
Thicker carotid intima–media thickness (CIMT) has been a valid predictor for atherosclerosis development. A significant association between environmental tobacco smoke (ETS) and thickening of CIMT has been demonstrated in adults, whereas such association has scarcely been reviewed in paediatric population. The dominate electronic databases, including MEDLINE (Ovid), PubMed, Embase, CINAHL, Web of Science, Scopus, were searched from inception.
Objective Patients with low-flow, low-gradient aortic stenosis (LFLG AS) and reduced left ventricular ejection fraction (LVEF) are known to suffer from poor prognosis after transcatheter aortic valve implantation (TAVI). This study aimed to develop a simple score system for risk prediction in this vulnerable subset of patients. Methods All patients with LFLG AS with reduced EF and sufficient CT data for aortic valve calcification (AVC) quantification, who underwent TAVI at five German centres, w
Objective Patients with low-flow, low-gradient aortic stenosis (LFLG AS) and reduced left ventricular ejection fraction (LVEF) are known to suffer from poor prognosis after transcatheter aortic valve implantation (TAVI). This study aimed to develop a simple score system for risk prediction in this vulnerable subset of patients. Methods All patients with LFLG AS with reduced EF and sufficient CT data for aortic valve calcification (AVC) quantification, who underwent TAVI at five German centres, w
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content