This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Jesse McLaren explains his AFIB mnemonic for approach to atrial fibrillation that involves 4 questions: 1. Is it atrial fibrillation? 2. If it is atrial fibrillation and there is rapid ventricular response, is it fast from a secondary cause? 3. If it is atrial fibrillation with a rapid ventricular response without a secondary cause, what is the intervention?
In late 2018 through 2020, The American Board of Internal Medicine (ABIM) was involved in a class action antitrust lawsuit for claims of illegal creation and maintenance of their monopoly power in the market for maintenance of certification (MOC).
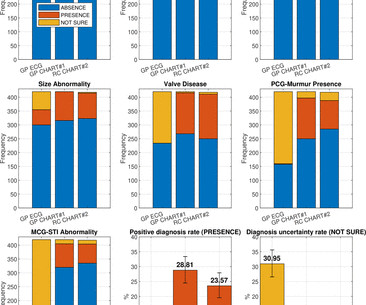
Purpose In a comparator study, designed with assistance from the Food and Drug Administration, a State-of-the-Art (SOTA) ECG device augmented with automated analysis, the comparator, was compared with a breakthrough technology, Cardio-HART (CHART). Methods The referral decision defined by physician reading biosignal-based ECG or CHART report were compared for 550 patients, where its performance is calculated against the ground truth referral decision.
A young man had an accidental exposure to carbon monoxide (CO). He was comatose and intubated and his initial Carboxyhemoglobin level was over 50%. An ECG is always recorded for CO toxicity. This was his ECG. It was shown to me with worry for ischemic ST elevation, which is certainly possible from severe CO toxicity, or concomitant ACS. In fact, there is laboratory evidence that CO toxicity increases Plateletneutrophil aggregates and plasma myeloperoxidase (MPO) concentration and thus may precip
Speaker: Simran Kaur, Co-founder & CEO at Tattva Health Inc.
AI is transforming clinical trials—accelerating drug discovery, optimizing patient recruitment, and improving data analysis. But its impact goes far beyond research. As AI-driven innovation reshapes the clinical trial process, it’s also influencing broader healthcare trends, from personalized medicine to patient outcomes. Join this new webinar featuring Simran Kaur for an insightful discussion on what all of this means for the future of healthcare!
Webinar Dos and Don’ts of the Mobile ECMO Team kchalko Thu, 02/17/2022 - 12:54 March 3, 2022 In this episode of the STS Webinar Series, a multidisciplinary panel shares their expertise in establishing and maintaining an effective mobile ECMO unit. In addition to optimal staffing, logistical details, and contingency plans for transport, the panel discusses findings from research on ECMO-facilitated resuscitation and contraindications for deploying the mobile ECMO unit.
Back in 2017, nearly a decade into my clinical training, I had just finished a difficult overnight cardiology shift managing critically ill patients with advanced cardiovascular disease. As I rode the New York City subway back to my upper west side apartment recounting the patients I had managed, and the decisions I had made that night, a lingering thought began growing.
In this Journal Jam podcast we dig deep into the science of FDA-approved outpatient medications for COVID with 3 critical appraisal masters: Dr. Andrew Morris, Dr. Rohit Mohindra and Dr. Justin Morgenstern. What is the evidence for the neutralizing monoclonal antibody medications like Sotrovimab? The nucleoside analogs like Remdesivir and Paxlovid? The inhaled corticosteroids like Budesonide and Ciclesonide?
In this Journal Jam podcast we dig deep into the science of FDA-approved outpatient medications for COVID with 3 critical appraisal masters: Dr. Andrew Morris, Dr. Rohit Mohindra and Dr. Justin Morgenstern. What is the evidence for the neutralizing monoclonal antibody medications like Sotrovimab? The nucleoside analogs like Remdesivir and Paxlovid? The inhaled corticosteroids like Budesonide and Ciclesonide?
The World Health Organization reports that cardiovascular disease is the leading cause of death worldwide [1]. One of these diseases is heart failure – a condition in which the heart is unable to pump enough blood to the organs in our body. This results in a deficiency of oxygen and nutrients in the cells of the body, which can have a huge impact on how it functions.
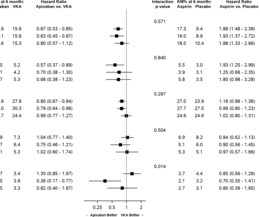
Objective Managing antithrombotic therapy in patients with atrial fibrillation (AF) and an acute coronary syndrome (ACS) and/or percutaneous coronary intervention (PCI) is challenging and can be affected by prior oral anticoagulant (OAC) treatment. We examined the relationship between prior OAC use and outcomes in the AUGUSTUS trial. Methods This prespecified secondary analysis is from AUGUSTUS, an open-label, 2-by-2 factorial, RCT to evaluate the safety of apixaban versus vitamin K antagonist (
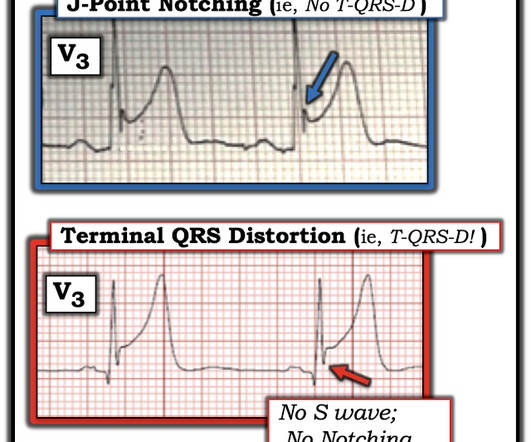
A 40 something otherwise healthy man presented with substernal chest pain. It had occurred once 3 days prior and resolved without any medical visit. He had a triage ECG at time zero: Here is the computer interpretation (Normal) This was the Veritas algorithm. What do you think? This ECG is DIAGNOSTIC of acute LAD Occlusion. The T-waves are hyperacute, but most important, the minimal ST Elevation is accompanied by Terminal QRS Distortion , or at least nearly so.
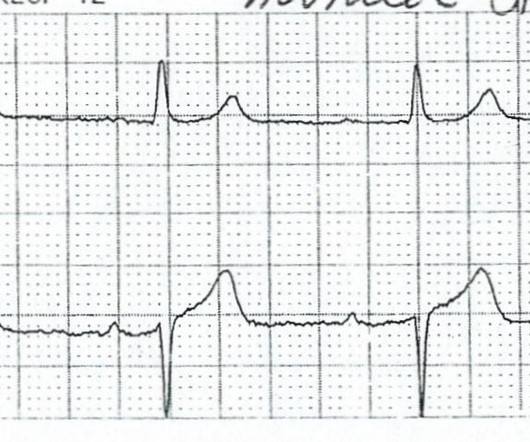
This two-lead rhythm strip shows a normal sinus rhythm at about 63 bpm. The P waves are regular. After the sixth P-QRS, there is a non-conducted P wave. The normal rhythm then resumes. The two most common reasons for a non-conducted P wave in the midst of a normal sinus rhythm are 1) non-conducted PAC, and 2) Wenckebach conduction. The first is easy to rule out.
It has been a long time since I have written anything concerning the American Board of Medical Specialties' (ABMS) Maintenance of Certification (MOC) board re-certification program. But when I read pieces in the media, like the one recently published in Medscape that spin the soothing narrative that MOC can become "kinder and gentler," I feel the need to speak out.
Diabetic nephropathy (DN) is the most common complication of diabetes mellitus. Although G protein subunit beta 4 (GNB4)-derived circular RNA (circ-GNB4; hsa_circ_0068087) is a promising candidate biomarker in diabetes mellitus, whether circ-GNB4 participates in DN occurrence and development remains unknown. Herein, we focused on DN-associated human renal mesangial cells (HRMCs) injury, and HRMCs were exposed in high glucose (HG) condition.
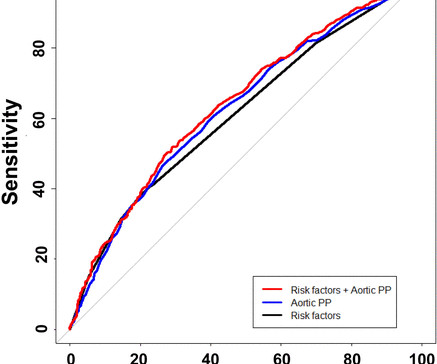
Background Pulse pressure (PP), a raw index of arterial stiffness, is inversely related to coronary microvascular function, even among patients with non-obstructive coronary artery disease (CAD), as per non-invasive studies. We aimed to determine whether invasive aortic PP is associated with coronary microvascular endothelial dysfunction (CMED) and/or coronary microvascular endothelial independent dysfunction (CMEID) in patients with non-obstructed CAD.
Webinar Coronary Revascularization Guideline: Why STS and AATS Did Not Endorse kchalko Thu, 02/10/2022 - 12:47 February 17, 2022 Senior leaders from STS and the American Association for Thoracic Surgery discuss the concerns that informed the decision not to endorse the 2021 Guideline for Coronary Artery Revascularization published in December by the American College of Cardiology, American Heart Association, and Society for Cardiovascular Angiography and Interventions.
This is written and contributed by Jesse McLaren (@ECGCases), with comments and edits by Smith, and commentary by Ken Grauer (@EKGPress) An 80 year-old female presented with weakness and a fall, with normal vitals and no injuries. The ECG was labeled ‘normal’ by the computer (Marqette 12SL), later confirmed by the cardiologist. What do you think? There’s normal sinus rhythm, normal conduction, normal axis, normal R wave progression, and normal voltages.
How many civil actions against Emergency Physicians does CMPA handle and what have been the outcomes? What are the 4 aspects of medical negligence and the anatomy of a legal action against physicians in Canada? What are the 3 stages of civil action in a medicolegal law suit in Canada? How should you respond when you are served with a medicolegal action?
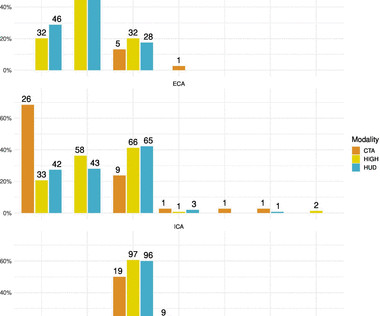
Objectives To investigate the reliability and agreement of hand-held ultrasound devices (HUDs) compared with conventional duplex ultrasound (HIGH) in examination for carotid stenosis in patients with suspected transitory ischaemic attack (TIA) or ischaemic stroke. Methods Cardiologists, experienced in carotid ultrasound, examined patients admitted to a community hospital with suspected stroke or TIA.
Background Disturbances of copper (Cu) homeostasis can lead to hypertrophic cardiac phenotypes (eg, Wilson’s disease). We previously identified abnormal Cu homeostasis in patients with hypertrophic cardiomyopathy (HCM) and, therefore, hypothesised that Cu 2+ –selective chelation with trientine dihydrochloride may slow or reverse disease progression in HCM.
A middle-aged man was found outside in the cold in full arrest in ventricular fibrillation. Chest compressions and ventilation were begun. On arrival, CPR was continued and core temperature was measured at 18° C (64.4° F). The patient was put on Extracorporeal Life Support in the ED 3 hours after initial resuscitation, the core temp was 30° C and the patient was defibrillated with a single attempt.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content